All published articles of this journal are available on ScienceDirect.

Single Centre Experience with Anaconda Custom-made Fenestrated Stent Graft in the Endovascular Repair of the Juxtarenal Aneurysms
Authors Info & Affiliations
Abstract
Aim:
The fenestrated Anaconda custom-made stent graft is one of the recently widely accepted fenestrated devices for managing complex juxta- and pararenal aortic pathology. This study showed its feasibility for treatment of challenging juxtarenal anatomy of the abdominal aorta.
Methods:
Over the period of 12 months, 9 patients with juxtarenal aortic aneurysm underwent fenestrated stent graft implantation in our institution. The graft fenestrations were customized on the basis of computerized tomography (CT-Angiography; CTA). Selected visceral ostia were protected with covered balloon-expandable stents after partial stent graft deployment. The perioperative and short term data were collected prospectively.
Results:
The mean aneurysm diameter was 58.4 mm (range 46-73 mm). The mean infrarenal neck length was 3.5 mm (range 0-7 mm), no patient had a severe (>60°) angulation of proximal neck. 18 fenestration for renal arteries, 1 for SMA and 3 for coeliac´s were treated with Advanta V12 covered stent. All the target vessels were cannulated successfully through fenestrations and all the stent grafts were successfully deployed in patients with no technical issue in the release mechanism. All the patients have undergone 6 month follow-up, no aneurysm related or aneurysm-unrelated deaths were reported. On the CTA scan, 3 of the patients had a weak type IIb endoleak; no type I or Type III endoleak was demonstrated. All target vessels were open without an instance of branch-stent stenosis/occlusion. No reintervention was needed.
Conclusion:
The usage of custom-made Anaconda fenestrated stent graft for endovascular treatment of juxtarenal aortic aneurysms is feasible with acceptable intermediate-term results.
1. INTRODUCTION
Despite improvements in EVAR (endovascular aortic repair) technology and decided advantage in perioperative morbidity and mortality, a hostile aneurysm anatomy including short (<15 mm) and angulated (>60°) proximal neck, inclusion of visceral branches and narrow vessels are limiting factors for this technique [1]. Surgical repair, in this setting, is more challenging than infrarenal aneurysm, as many will require suprarenal or supraceliac clamping, which has been associated with a greater blood loss, and potentially worse outcomes. In order to overcome this problem, fenestrated and branched grafts were developed, allowing the use of the visceral segment as a landing zone with continual perfusion of renal and visceral vessels [2]. In 1999, the first of these devices was successfully implanted [3]. Many studies have demonstrated fenestrated endovascular aortic repair (FEVAR) as a successful treatment of complex juxtarenal aortic aneurysm with lower overall mortality compared with open repair, as well as high immediate and midterm target vessel patency rates with a low rate of secondary interventions [4-6].
We report our experience with custom-made Anaconda fenestrated stent graft (Vascutek, Inchinnan, United Kingdom) in patients with complex juxtarenal aortic aneurysm anatomically unsuitable for conventional EVAR.
2. MATERIALS AND METHODS
2.1. Patient Selection
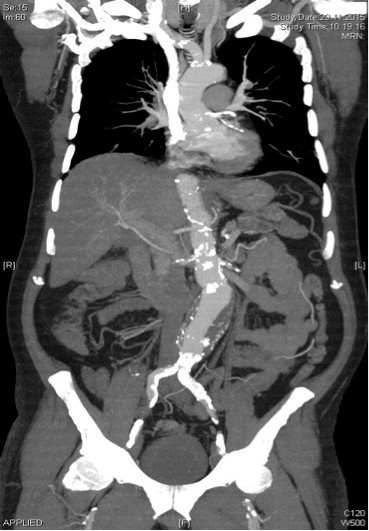
Between January 2015 and July 2016, 9 patients with asymptomatic juxtarenal aortic aneurysm received an Anaconda fenestrated stent graft. The indications for fenestrated graft in complex aneurysms were a maximum aneurysm diameter >5 cm and unfavourable proximal neck anatomy (length <1 cm, conical). All the patients underwent preoperative multislice high- resolution Computed Tomographic Angiography (CTA) (Fig. 1). Three dimensional and multiplanar workstation reconstructions (TeraRecon, Foster City, CA, USA) were performed to evaluate the aneurysm anatomy and to plan graft dimensions. Devices were customized to include all those vessels regarded as essential for the target organ function.
2.2. Anaconda Fenestrated Stent Graft
The custom-made Anaconda system has been previously described in detail [1] (Fig. 2). The system consists of 3 separate components: the main aortic body and 2 separate iliac legs. The proximal end of the main body has 2 separate nitinol rings separated by a distance of 8 to 11 mm. To provide an auxiliary sealing function, 4 “pairs” of nitinol hooks protrude in a caudal direction from the inferior ring. The depth of the valley can be adjusted dependent on the oversize between native aorta and the ring stent diameter or, in the case of augmented anterior valley/scallop. The fenestration is placed in an unsupported region of the graft body, which facilitates treatment of angulated necks. One of the most important advantages of the graft is its repositionability. Hence, even after cannulation of target vessels and unsheathing of the device in partially deployed state, the operator is still able to reposition the stent graft.

2.3. Stent Graft Planning
CTA images were imported into TeraRecon workstation for planning the fenestrated Anaconda stent graft. Orientation, angulation, and size target vessel ostia, aneurysm neck length, diameter, and angulation, the position of aortic bifurcation as well as the iliac anatomy were all considered. To verify the correct positioning of the fenestrations, prototype grafts in silicone aortic models were developed.
2.4. Graft Implantation
All of the procedures were performed in the operating room using a C-arm with patients under general anesthesia. Bilateral common femoral arteries were exposed surgically in all cases. All the patients received 5000 IU of heparin immediately prior to artery cannulation, with additional boluses to keep the activated clotting time at 250 sec. The main body was then positioned by laterally oriented “peaks” above the renal arteries and the “valleys” of the proximal end of the main body were oriented anteroposteriorly depending on the position of the superior mesenteric artery or celiac artery. The main body was deployed and the target vessels were cannulated with a subsequent Advanta V12 (Atrium, Hudson, NH) balloon-expandable covered stent placement and flaring proximally (Fig. 3). The implantation of iliac legs bilaterally with the subsequent balloon dilatation finalized the procedure. Completion angiography was performed to ensure adequate exclusion of the aneurysm and the absence of endoleak or target-vessel obstruction.

2.5. Follow-up
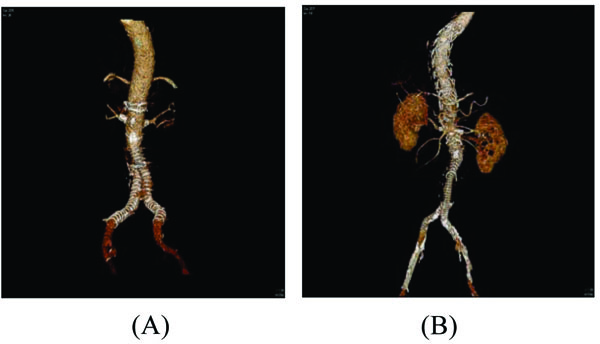
After the procedure, all the patients were transferred to the intensive care unit to provide invasive arterial and central venous monitoring, as well as assessment of the renal function. Following discharge, all the patients were entered into our surveillance program with a follow-up at 6 months, 1 year (Figs. 4a and 4b) and yearly thereafter with CTA and renal function testing.
2.6. Statistical Analysis
Statistical analysis was performed using SPSS 19 software package for Windows (SPSS Inc., Chicago, Illinois, USA). Distribution of data was primarily assessed by visual analysis of histogram. Normally distributed data were analysed either with the Student t-test for continuous or Pearson’s chi-2 test for dichotomous variables. A p <0.05 was considered significant.
3. RESULTS
3.1. Demographics and Aneurysm Morphology
Over the period of 16 months, 9 Anaconda fenestrated grafts were performed on patients who met appropriate indication for fenestrated EVAR. The patients (6 men, 3 women) had a mean age of 75.4 years (range: 70-88 years). The patients were of American Society of Anesthesiology (ASA) grade III, and comorbidities are listed in Table 1. The mean infrarenal neck length was 3.5 mm (range 0-7 mm), no patient had a severe (>60°) angulation of proximal neck or thrombus involving more than two-thirds of the proximal landing zone diameter. The mean aneurysm diameter was 58.4 mm (range 46-73 mm).
| Patient | Age, Years | Gender | Comorbidities | Serum Creatinine µmol/l |
ASA |
|---|---|---|---|---|---|
| 1 | 88 | M | Smoker, Hypercholesterolaemia | 141 | III |
| 2 | 80 | F | Ischaemic heart disease, Hypertension, COPD, Hypercholesterolaemia | 126 | III |
| 3 | 75 | M | Ischaemic heart disease, Congestive heart failure, Hypertension, Smoker, Hypercholesterolaemia | 75 | III |
| 4 | 74 | M | Hypertension, Hypercholesterolaemia | 108 | III |
| 5 | 71 | F | Hypertension, COPD, Hypercholesterolaemia | 64 | III |
| 6 | 73 | F | Hypertension | 69 | III |
| 7 | 73 | M | Hypertension, Hypercholesterolaemia | 71 | III |
| 8 | 70 | M | Ischaemic heart disease, Hypertension, COPD, Diabetes mellitus, Smoker, Hypercholesterolaemia | 137 | III |
| 9 | 75 | F | Ischaemic heart disease, Congestive heart disease, Hypertension, Smoker, Hypercholesterolaemia | 70 | III |
| Patient | Infrarenal Neck Length (mm) | AAA Diameter (mm) | Previous Aortic Intervention | Radiation Time/min. | Contrast Volume/ml | Major Complication (Spinal Cord Ischaemia, Hemiparesis/-plegia, Acute Renal Failure, Stroke, Myocardial Infarction, Limb Ischaemia) | Hospital Stay (days) |
|---|---|---|---|---|---|---|---|
| 1 | 9 | 73 | n | 63 | 64 | n | 19 |
| 2 | 7 | 60 | n | 66 | 68 | n | 16 |
| 3 | 5 | 51 | n | 59 | 60 | n | 17 |
| 4 | 4 | 58 | n | 52 | 48 | n | 7 |
| 5 | 5 | 69 | n | 99 | 100 | n | 7 |
| 6 | 8 | 46 | EVAR | 56 | 48 | n | 8 |
| 7 | 7 | 66 | n | 61 | 62 | n | 10 |
| 8 | 9 | 52 | TEVAR | 78 | 88 | Acute right leg ischaemia with thrombosis of the femoral artery | 30 |
| 9 | 8 | 51 | n | 24 | 86 | n | 8 |
| Patient | AAA Diameter (mm) Preoperatively | AAA Diameter (mm) 6 Months Postoperatively |
Endoleak | Reintervention | Fenestration (open, stenosis, closed) | Serum Creatinine µmol/l |
|---|---|---|---|---|---|---|
| 1 | 73 | 71 | IIb | n | Open/no stenosis | 132 |
| 2 | 60 | 57 | n | n | Open/no stenosis | 200 |
| 3 | 51 | 51 | IIb | n | Open/no stenosis | 76 |
| 4 | 58 | 55 | n | n | Open/no stenosis | 108 |
| 5 | 69 | 66 | n | n | Open/no stenosis | 73 |
| 6 | 46 | 46 | n | n | Open/no stenosis | 80 |
| 7 | 66 | 66 | IIb | n | Open/no stenosis | 81 |
| 8 | 52 | 49 | n | n | Open/no stenosis | 148 |
| 9 | 51 | 43 | n | n | Open/no stenosis | 57 |
3.2. Graft Implantation
18 Fenestration for renal arteries, 1 for SMA (superior mesenteric artery) and 3 for truncus coeliacus were treated with Advanta V12 covered stents. All target vessels were cannulated successfully trough fenestrations, and all the branch vessels remained perfused after the procedure. All of the Advanta V12 stents were flared at the fenestration to create a sealing zone between the Advanta stent and Anaconda prosthesis. Mean radiation time was 62 min (range: 24-99 min) and a mean of 69.3 ml of iodinated contrast (range, 48-100 ml) was used per case. All the stent grafts were successfully deployed in patients with no technical issue in the release mechanism. Completion of DSA (digital subtraction angiography) showed successful exclusion of the aneurysm in all cases, with no reintervention needed on any branch-stent.
3.3. Morbidity and Mortality
The 30-day mortality was 0%. Perioperative morbidity included an acute ischaemia of the right leg due the thrombosis of common femoral artery in 1 patient and groin lymphocele in 3 patients. The mean length of stay was 13.6 days (range: 7-30 days) (Table 2). There was a significant difference between preoperative and postoperative creatinine levels (p=0.004; Pearson correlation test).
3.4. Follow-up
All the patients have undergone 6 months follow-up, no aneurysm related or aneurysm-unrelated deaths have been reported. On the CTA scan, 3 of the patients had a weak type IIb endoleak, no type I or Type III endoleak was demonstrated. All the target vessels were open without an instance of branch-stent stenosis/occlusion. Renal function remained unchanged. Only one patient had a 33% increase in creatinine due to acute kidney injury because of multiple CT-scans in accordance with his femur fracture 3 months after the FEVAR. No reintervention was needed (Table 3).
4. DISCUSSION
This article described our experience with fenestrated custom-made Anaconda graft in complicated juxtarenal aortic anatomy. Although the most common used, fenestrated graft, is the Cook Zenith (Cook Medical) [7], due to the possibility to cannulate from a brachial approach, in cases of severe neck angulation and feasibility to reposition the graft, we decided to use the Anaconda fenestrated device for our patients [8]. The early results of this study of 9 patients showed successful aneurysm exclusion without type I or III endoleak.
We appreciate the repositioning of the Anaconda custom-made fenestrated graft. After the device is unsheathed, it can be partially collapsed and again anatomically correctly placed. This option enables accurate deployment with respect to the renal and visceral arteries and allows easy correction of any mismatch between fenestrations and target vessels. The repositionable stent graft with unsupported body- below the proximal sealing stents consists the main body of the unsupported fabric – might support during cannulation of target vessel with challenging anatomy i.e. in severe angulated neck. Additionally, the unsupported main body simplifies planning and manufacture of the fenestrations in the size or position.
The use of Anaconda custom fenestrated graft has been described in many studies with successful application and promising, short , as well as intermediate (1 and 6 months) outcomes [8, 9]. Colgan et al. used the custom-made fenestrated Anaconda aortic stent graft in a recently published UK multicentre study; they reported a low procedural mortality and a high rate of technical and clinical success at 30 days and 1 year [10]. In our study with small numbers and intermediate follow-up period, we also noted a successful implantation of the fenestrated Anaconda stent graft with no Type I or III endoleak, no occlusion/stenosis in the branches, as well as no morbidity or mortality periprocedurally and in the 6 months follow-up.
The aim of this study is to demonstrate the Anaconda custom-made fenestrated graft as an option with low perioperative mortality rates compared with open surgery in juxtarenal aortic aneurysms with complex anatomy. Each stent graft needs to be planned individually for the patient in collaboration with the manufacturer. Furthermore, the implantation of fenestrated stent graft requires expertise and should be performed in a centre with experience in stent graft technology.
CONCLUSION
Nine patients underwent Anaconda custom-made fenestrated stent graft placement. In all the cases, the deployment was technically successful. Unsupported and repositionable Anaconda main body, as well as ante- or retrograde cannulation of target vessels comprises the main advantages of this graft. Intermediate term results are promising regarding endoleak, target vessel and low periprocedural complications. Long-term results remain to be established in terms of durability of this system.
LIST OF ABBREVIATIONS
| TEVAR | = Thoracic Endovascular Aortic Repair |
| EVAR | = Endovascular Aortic Repair |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals / humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIAL
The data supporting the findings of the article is not freely availaible due to laws and regulations governing mediacal data protection and security. To get more information regarding the data please contact the corresponding author Milan Lisy, MD.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

