All published articles of this journal are available on ScienceDirect.

ST-Segment Elevation During Treadmill Exercise Test in a Patient without Prior Myocardial Infarction. A Case Report and Literature Review
Authors Info & Affiliations
Abstract
Exercise-induced ST-elevation is extremely uncommon especially in patients without prior myocardial infarction. It is more common among post-infarction patients with Q waves on the resting ECG. In the current case we report a 50-year-old man with a history of chest pain on exertion started four months ago. During the exercise test, ST-elevation was observed in leads II, III, AVF. Coronary angiography revealed significant stenoses in the right coronary artery and left circumflex artery, which were treated with percutaneous coronary intervention. This case highlights the rare finding of exercise-induced ST-elevation and reviews possible mechanisms.
1. INTRODUCTION
Exercise stress testing has been regarded as the optimum method for the identification of myocardial ischemia. Nowadays, the method sensitivity as well as, specificity in the confirmation of ischemia has been greatly enhanced both by complying with more standardized protocols and the advance of mechanical equipment [1].
2. CASE REPORT
A 50-year-old gentleman presented to outpatient clinic with effort angina starting 4 months ago (Class III Canadian Cardiovascular Society). He had a positive family history of CAD and hypercholesterolemia treated with statins. He was an active smoker, with normal body mass index and no additional cardiovascular risk factors. Resting ECG was normal. Cardiac examination revealed a regular rhythm with no additional heart sounds.
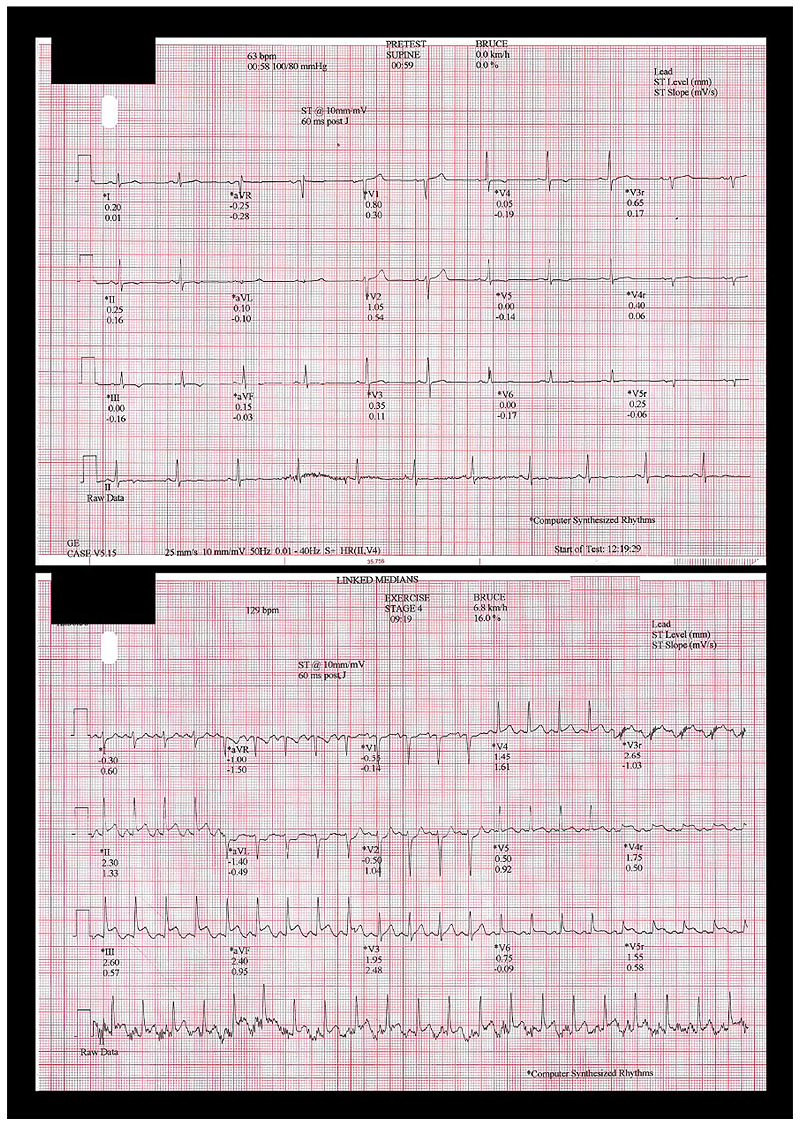
The patient was subjected to treadmill exercise test using the BRUCE protocol. The patient's vital signs were measured prior to the exercise test and were found to be normal (blood pressure: 120/70mmHg; heart rate: 68bpm). During the ninth minute of the test, 2mm ST-elevation was observed in leads II, III, AVF with ST-depression in leads I, AVL (Fig. 1). The patient experienced severe chest pain. The test was immediately stopped and electrocardiographic recording continued during recovery. Blood pressure just before the was 150/80 mmHg and heart rate was 131bpm (8 METs, 91% of maximal age-predicted). During the first three minutes of the recovery, ST-elevation was resolved and the symptoms improved without medical intervention. The patient was transferred to the Cath-lab for urgent coronary angiography.
3. DISCUSSION
Exercise stress testing is being used for more than 6 decades, in order to identify myocardial ischemia. Multiple studies have shown that a cut-off point of 0.1mV (1mm) horizontal or downsloping ST-segment depression has 68% sensitivity and 77% specificity [2]. Exercise-induced ST-elevation is uncommon, and more commonly occurs in post-infraction patients with pre-existing Q waves on the resting ECG, due to possible reversible ischemia in the peri-infarct area or left ventricular wall motion abnormalities at rest [3]. For patients without previous MI and Q waves on the resting ECG, exercise-induced ST elevation is more unusual. Data from 14,941 exercise stress tests performed in patients with chest pain and without previous MI revealed that ST elevation occurred only in a small percentage (0.78%- 116 patients). Most patients (60.3%) developed ST elevation in stages 1 or 2 of the Bruce protocol. Of those who developed ST-elevation during the exercise phase, all but one persisted during the recovery period. Also, 56 patients terminated the test due to chest pain. All 108 patients, who underwent coronary angiography had at least one severe lesion [4].
Various pathogenetic mechanisms have been suggested regarding ST-elevation during exercise stress test. Data from 6,147 patients without MI who underwent exercise stress test, with only 9 patients demonstrating ST-elevation, concluded that coronary vasospasm was the most common underlying pathology [5]. Recent studies are implicating severe coronary artery stenosis as the mechanism of exercise-induced ST-elevation. Among 29,002 patients undergoing stress myocardial perfusion imaging, only 39 (0.13%) developed ST-elevation. Of those, the majority had significant coronary artery disease, 87% had >90% stenosis, and 59% had multi-vessel disease [3]. Murphy J. et al. [4] mentioned that ST segment elevation during stress test is due to severe coronary artery stenoses as an almost exclusive cause and highlighted the worldwide regional differences in aetiology of this finding. Indeed, only one of the patients who enrolled in the study had short-lived ST elevation with exercise that resolved with an increasing workload and may have been attributed to coronary artery spasm [4]. In our case, exercise-induced ST-elevation was due to severe obstruction and not only due to coronary spasm. Although it is unclear whether ECG changes can identify the culprit artery [3, 6], in our case the culprit lesion co-localized with the ECG changes, in line with observations by Beinart et al. [3]
In conclusion, ST-elevation during exercise stress test is rare, but has significant predictive value. Urgent coronary angiography should be performed for further diagnosis and management.
Coronary angiography revealed 80% stenosis in the RCA and 75% stenosis in the left circumflex artery. (Fig. 2) Neither thrombus, nor angiographic evidence of plaque rupture was detected. During coronary angiography, the patient received intracoronary nitrites without improving the angiographic grade of the stenosis. The patient underwent PCI of the RCA lesion using a 3.5x15mm drug eluting stent with good angiographic result and TIMI III flow. The ST-segment elevation improved after coronary angioplasty. The patient remained hemodynamically stable in the coronary care unit without arrhythmia, and was discharged four days later. Echocardiography showed normal left ventricular dimensions with inferior and posterior wall motion abnormalities (ejection fraction 45%).

LIST OF ABBREVIATIONS
| CAD | = Coronary Artery Disease |
| ECG | = Electrocardiography |
| RCA | = Right Coronary Artery |
| TIMI | = Thrombolysis In Myocardial Infarction |
| PCI | = Percutaneous Coronary Intervention |
| MI | = Myocardial Infarction |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all the participants.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

