All published articles of this journal are available on ScienceDirect.

Midwall Fibrosis: Cardiac Magnetic Resonance Imaging in Risk Stratifying Cardiomyopathies
Authors Info & Affiliations
Abstract
The United Kingdom’s National Institute for Health and Care Excellence guidance on implantable cardiac defibrillator (ICD) therapy recommend ICD in those with left ventricular dysfunction and a high risk of sudden cardiac death (SCD). SCD accounts for 30% deaths in non-ischaemic dilated cardiomyopathy (DCM), however risk stratifying and predicting SCD in DCM is a major management challenge. We present two cases demonstrating the potential role of cardiac magnetic resonance imaging in risk stratifying DCM.
INTRODUCTION
A 35 year old gentleman presented with haemodynamically unstable ventricular tachycardia (VT) which required DC cardioversion. Coronary angiography demonstrated normal epicardial vessels. Plain chest radiograph, serum ACE, Ca2+ and alpha-galactosidase were normal. Cardiac biopsy was not performed. Cardiac magnetic resonance (CMR) scan revealed extensive mid wall late gadolinium enhancement (LGE) and normal T2 weighted images (Fig 1). An implantable cardiac defibrillator (ICD) was inserted for secondary prevention.
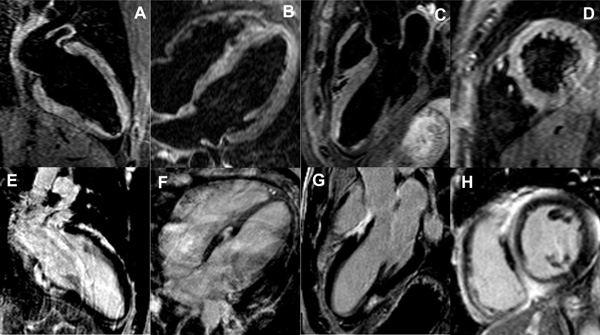
Normal T2 imaging (A-D) and extensive mid myocardial wall late gadolinium enhancement (E-H) in the long and short axis views.

Dilated cardiomyopathy with mid myocardial late gadolinium enhancement in short axis (A) and horizontal long axis (B) views.
A further patient presented with breathlessness (New York Heart Association Classification III) and palpitations. There was no history of syncope or family history of sudden cardiac death (SCD). Coronary angiography was normal. CMR demonstrated severe left ventricular systolic dysfunction (ejection fraction [EF] 21%) with extensive mid wall LGE (Fig 2). Cardiac resynchronization therapy defibrillator (CRT-D) was implanted for primary prevention.
Case 1 illustrates an established example for the role of an ICD for secondary prevention whilst case 2 illustrates a potential role for CMR in risk stratification dilated cardiomyopathy for primary prevention. The United Kingdom’s National Institute for Health and Care Excellence guidance on ICD implantation for primary prevention recommend ICD in those with left ventricular (LV) dysfunction (LV EF ≤ 35%) in those with a high risk of SCD [1]. SCD accounts for 30% deaths in non-ischaemic dilated cardiomyopathy (DCM) and risk stratifying and predicting SCD in this group is a major management challenge. Although limited to two cases, we demonstrated how cardiac magnetic resonance may help in risk stratification prior to ICD implantation. Mid wall fibrosis has been shown to have prognostic value, predicting both VT and SCD [2, 3], however is not currently incorporated into any guideline for ICD implantation. Furthermore, current guidelines consider DCM as a homogenous entity and tissue characterisation by multi-parametric CMR can differentiate the cause.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
DPR and OEG acknowledge the support of the Gawthorn Cardiac Trust

