All published articles of this journal are available on ScienceDirect.

Angiotensinogen (AGT) M235T, AGT T174M and Angiotensin-1- Converting Enzyme (ACE) I/D Gene Polymorphisms in Essential Hypertension: Effects on Ramipril Efficacy
Authors Info & Affiliations
Abstract
Background:
Hypertension, one of the most important risk factors for premature cardiovascular disease, is a major worldwide public health problem. Angiotensin-1-converting enzyme (ACE) and angiotensinogen (AGT) gene polymorphisms are thought to be associated with primary hypertension. In the present study, we examined the frequency of these gene polymorphisms in an adult population with and without essential hypertension. Furthermore, we evaluated the effect of ACE and AGT gene polymorphisms on ramipril treatment efficacy in the hypertensive patients.
Methods:
A total of 166 adults (83 hypertensives and 83 normotensives) were involved in the study and genotyped for AGTM235T (rs699), AGTT174M (rs4762) and ACEI/D (rs1799752) gene polymorphisms.
Results:
The genotype and allele distribution of the AGTM235T variant significantly differed between hypertensives and normotensives [odds ratio (OR) = 1.57% (T vs M allele), 95% confidence intervals (CIs): 1.01 - 2.44; p=0.045 for hypertensives]. However, none of the 3 studied Simple Nucleotide Polymorphisms were associated with the blood pressure-lowering response to ramipril.
Conclusion:
These results suggest that AGTM235T gene polymorphism is associated with essential hypertension. However, none of the AGTM235T, AGTT174M and ACEI/D gene polymorphisms influenced ramipril effectiveness.
INTRODUCTION
Despite numerous antihypertensive agents, hypertension is still not adequately controlled [1-3]. This can be attributed to a combination of psychosocial, socio-economic, environmental and physician-related effects, but also to a genetic predisposition. The genetic influence of blood pressure (BP) variation is expected to be approximately 30-40% [4, 5]. Until now, more than 150 candidate genes have been associated with BP regulation. In this context, genes such as angiotensinogen (AGT) and angiotensin-1-converting enzyme (ACE), which encode proteins of the renin-angiotensin system (RAS) have been widely evaluated [6, 7].
AGT is the natural substrate of RAS produced in the liver. The associations of these variants are contradictory in different populations [8]. The AGT gene is located at lq42-43 and consists of 5 exons and 4 introns spanning 13 kb [9]. The AGT gene is a logical candidate for BP control, taking into consideration the strong correlation between plasma AGT levels and BP [10]. Although several polymorphisms in the AGT region have been recognized [11], a special focus has been focused on 2 polymorphisms, M235T (rs699) and T174M (rs4762), both found in exon 2.
ACE is a key zinc metallo-enzyme of the RAS widely allocated in the kidney [12]. ACE catalyzes the conversion of angiotensin I to the biologically active peptide, angiotensin II, which is involved in the control of fluid electrolyte balance and systemic BP [12]. This poly-morphism is characterized by the presence (insertion) or absence (deletion) of a 287 bp AluYa5 element inside intron 16. ACEI/D gene polymorphism has been associated with the presence of essential hypertension [13, 14].
Several antihypertensive drugs target RAS pathways such as ramipril, an ACE inhibitor, involved in the treatment of hypertension and congestive heart failure. In the present study, we evaluated the frequency of 3 Simple Nucleotide Polymorphisms (SNPs) such as AGTM235T (rs699), AGTT174M (rs4762) and ACEI/D (rs1799752) in hypertensive and normotensive individuals as well as the possible influence of these Single Nucleotide Polymor-phisms (SNPs) on ramipril-induced BP lowering.
PATIENTS AND METHODOLOGY
The present study was designed and performed in agreement with the recommendations for the human genotype-phenotype association studies published by the NCI-NHGRI (National Cancer Institute-National Human Genome Research Institute) Working Group on Replication in Association Studies [15] indicated time period and location of subject recruitment, success rate for DNA acquisition, internal control samples (from the same DNA) and sample tracking methods.
Subjects: A total of 166 participants were included in the present study divided into 2 groups. Control group (n = 83, 56 ± 20 years, 44 men): subjects were recruited from the outpatient clinics of the Orthopedic and Urologic Departments of the Veterans Administration Hospital (NIMTS). Inclusion criteria were: age 18 -<80 years, no history of coronary artery disease, diabetes mellitus, thyroid and liver disease, heart and renal failure, high alcohol consumption, professional athleticism and any chronic disease, hypertension or antihypertensive drug therapy and BP within normal limits according to current guidelines [16, 17].
Hypertensive group (n = 83, 67 ± 13 years, 48 men): newly-diagnosed hypertensive patients were randomly recruited from the Outpatient Clinic of the Onassis Cardiac Surgery Centre. Inclusion criteria were age 18 - < 80 years, no history of thyroid and liver disease, heart and renal failure, high alcohol consumption, and elevated BP (hypertension was defined as systolic BP >140 mmHg and/or diastolic BP >90 mmHg). These patients had no prior or current use of antihypertensive agents. BP was measured twice and the lower value was recorded. The measurement was performed on the right upper arm by auscultation method after the subject had been seated for at least 5 min. Mercury sphygmomanometers were used and the appropriate adult cuff size was applied. Secondary hypertension was excluded by the use of a detailed health questionnaire.
Written consent was obtained from each participant. The study protocol was approved by the institutional ethics committee (Onassis Cardiac Surgery Center, Athens, Greece) and was in accordance with the Declaration of Helsinki for Human Research of 1974 (last modified in 2000). All study cohorts were of Caucasian origin and descent for ≥3 generations.
RAMIPRIL ADMINISTRATION
We initially administered ramipril monotherapy in the hypertensive patients (dose ranged from 2.5 to 10 mg daily, according to BP values), followed by combination therapy (i.e. addition of a diuretic) if needed. The associations between genotypes of the 3 candidate genes and BP decrease by ramipril monotherapy were evaluated.
GENOTYPING
Genotyping was performed for research purposes. Extraction of genomic DNA was performed from leukocytes separated from whole blood using a standard method with Qiagen FlexiGene DNA kit.
The oligonucleotide primers used for AGTM235T (rs699) polymorphism were 5’-CCGTTTGTGCAGGGCCT GGCTCTC -3’ and 5’-CAGGGTGTCCACACTGGCTCG −3 as described by Bennett et al. [18]. Polymerase Chain Reaction (PCR) was subjected to 95 οC for 5 min, 30 cycles of 95οC for 30 s, 55οC for 30 s and 72οC for 30 s and final extension to 72οC for 7 min, producing a fragment of 165 bp. This fragment was subsequently cleaved by restriction enzyme BstUI (Bacillus stearothermophilus U458), creating fragments for T allele 141 bp and 24 bp and for M allele 165 bp, which were subjected to electrophoresis on an agarose gel 4% and visualized with ethidium bromide (Fig. 1).
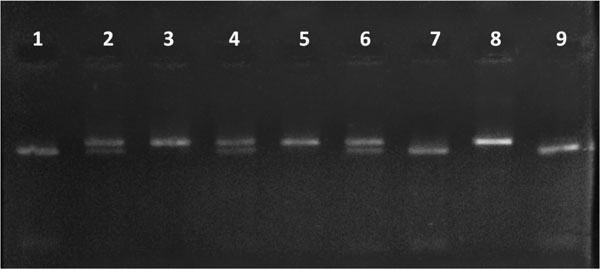
AGTM235T gene polymorphism. 1, 7, 9: TT genotype; 2, 4, 6: MT genotype; 3, 5, 6: MM genotype
Abbreviations: AGT: Angiotensinogen.
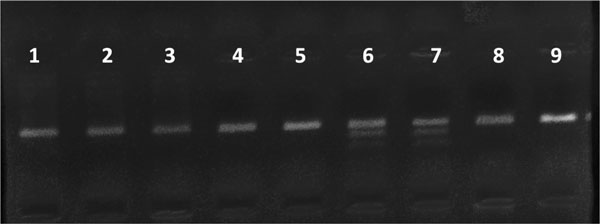
AGTT174M gene polymorphism. 1-5, 8, 9: TT genotype; 6, 7: TM genotype.
MM genotype was not detected in the study groups
Abbreviations: ACE: Angiotensin-1-converting enzyme.
Demographic data, clinical characteristics and lipid profile of the study groups.
| Group | |||||
|---|---|---|---|---|---|
| Control | Ramipril | ||||
| Categorical variables | N | % | N | % | |
| Gender | Men | 44 | 53.0% | 48 | 57.8% |
| Women | 39 | 47.0% | 35 | 42.2% | |
| CAD | Yes | 0 | 0.0% | 24 | 28.9% |
| No | 83 | 100.0% | 59 | 71.1% | |
| Stroke | Yes | 0 | 0.0% | 4 | 4.8% |
| No | 83 | 100.0% | 79 | 95.2% | |
| Smoking | Yes | 29 | 34.9% | 10 | 12.0% |
| No | 48 | 57.8% | 41 | 49.3% | |
| Ex | 6 | 7.2% | 32 | 38.6% | |
| Diabetes | Yes | 0 | 0.0% | 23 | 27.7% |
| No | 83 | 100.0% | 60 | 72.3% | |
| Continuous variables | Mean | Standard Deviation | Mean | Standard Deviation | |
| Age (yrs) | 56 | 20 | 67 | 13 | |
| BMI (kg/m2) | 24.5 | 3.1 | 27.7 | 3.8 | |
| TC (mg/dl) | 170 | 31 | 231 | 60 | |
| TG (mg/dl) | 82 | 26 | 164 | 147 | |
| HDL-C (mg/dl) | 48 | 13 | 49 | 15 | |
| LDL-C (mg/dl) | 107 | 28 | 146 | 50 | |
| Baseline DBP (mmHg) | 73 | 8 | 88 | 11 | |
| Baseline SBP (mmHg) | 123 | 12 | 159 | 18 | |
| DBP (mmHg) after treatment | 76 | 9 | |||
| SBP (mmHg) after treatment | 130 | 15 |
Abbreviations: CAD: coronary artery disease; BMI: body mass index; TC: total cholesterol; TG: triglycerides; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol, SBP: systolic blood pressure, DBP: diastolic blood pressure
Frequency of the 3 Simple Nucleotide Polymorphisms (SNPs) in study groups.
| Group | ||||||
|---|---|---|---|---|---|---|
| Control | Ramipril | |||||
| Count | Column N % | Count | Column N % | p | ||
| AGTM235T | MM | 30 | 36.1% | 23 | 27.7% | 0.042 |
| MT | 47 | 56.6% | 43 | 51.8% | ||
| TT | 6 | 7.2% | 17 | 20.5% | ||
| AGTT174M | TT | 70 | 84.3% | 65 | 78.3% | 0.319 |
| TM | 13 | 15.7% | 18 | 21.7% | ||
| MM | 0 | 0.0% | 0 | 0.0% | ||
| ACEI/D | II | 14 | 17.1% | 11 | 13.3% | 0.712 |
| ID | 38 | 46.3% | 43 | 51.8% | ||
| D | 30 | 36.6% | 29 | 34.9% | ||
| AGTM235 allele | M | 107 | 64.5% | 89 | 53.6% | 0.045 |
| T | 59 | 35.5% | 77 | 46.4% | ||
| AGTT174M allele | T | 153 | 92.2% | 148 | 89.2% | 0.346 |
| M | 13 | 7.8% | 18 | 10.8% | ||
| ACEI/D allele | I | 66 | 40.2% | 65 | 39.2% | 0.840 |
| D | 98 | 59.8% | 101 | 60.8% |
Abbreviations: AGT: Angiotensinogen; ACE: Angiotensin-1-converting enzyme.
Frequency of AGTM235T, AGTT174M and ACE I/D genotype polymorphisms and level of blood pressure [grade 1 HYP (hypertension), High normal, Normal, and Optimal) defined by the European Society of Cardiology in Hypertensive group [17].
| Blood Pressure | ||||||
|---|---|---|---|---|---|---|
| Grade 1 HYP | High Normal | |||||
| Count | Column N % | Count | Column N % | p | ||
| AGTM235T | MM | 7 | 33.3% | 13 | 25.0% | 0.770 |
| MT | 10 | 47.6% | 28 | 53.8% | ||
| TT | 4 | 19.0% | 11 | 21.2% | ||
| AGTT174M | TT | 16 | 76.2% | 41 | 78.8% | 0.999 |
| TM | 5 | 23.8% | 11 | 21.2% | ||
| MM | 0 | 0.0% | 0 | 0.0% | ||
| ACEI/D | II | 2 | 9.5% | 7 | 13.5% | 0.887 |
| ID | 11 | 52.4% | 27 | 51.9% | ||
| D | 8 | 38.1% | 18 | 34.6% | ||
| Blood pressure | ||||||
| High Normal | Normal | |||||
| Count | Column N % | Count | Column N % | p | ||
| AGTM235T | MM | 11 | 26.8% | 9 | 28.1% | 0.948 |
| MT | 22 | 53.7% | 16 | 50.0% | ||
| TT | 8 | 19.5% | 7 | 21.9% | ||
| AGTT174M | TT | 31 | 75.6% | 26 | 81.3% | 0.563 |
| TM | 10 | 24.4% | 6 | 18.8% | ||
| MM | 0 | 0.0% | 0 | 0.0% | ||
| ACEI/D | II | 5 | 12.2% | 4 | 12.5% | 0.223 |
| ID | 18 | 43.9% | 20 | 62.5% | ||
| D | 18 | 43.9% | 8 | 25.0% | ||
| Blood pressure | ||||||
| Normal | Optimal | |||||
| Count | Column N % | Count | Column N % | p | ||
| AGTM235T | MM | 17 | 28.8% | 3 | 21.4% | 0.736 |
| MT | 31 | 52.5% | 7 | 50.0% | ||
| TT | 11 | 18.6% | 4 | 28.6% | ||
| AGTT174M | TT | 47 | 79.7% | 10 | 71.4% | 0.721 |
| TM | 12 | 20.3% | 4 | 28.6% | ||
| MM | 0 | 0.0% | 0 | 0.0% | ||
| ACEI/D | II | 8 | 13.6% | 1 | 7.1% | 0.637 |
| ID | 29 | 49.2% | 9 | 64.3% | ||
| D | 22 | 37.3% | 4 | 28.6% | ||
Grade 1 hypertension (140-159 and/or 90-99 mmHg), High normal (130-139 and/or 85-89 mmHg), Normal (120-129 and/or 80-84 mmHg) and Optimal (<120/<80 mmHg).
Abbreviations: AGT: Angiotensinogen; ACE: Angiotensin-1-converting enzyme.
Allele Frequency of AGTM235T, AGTT174M and ACE I/D gene polymorphisms level of blood pressure [grade 1 HYP (hypertension), High normal, Normal, and Optimal) defined by the European Society of Cardiology in Hypertensive group [17].
| Blood Pressure | ||||||
|---|---|---|---|---|---|---|
| Grade 1 HYP | High Normal | |||||
| Count | Column N % | Count | Column N % | p | ||
| AGTM235T | M | 24 | 57.1% | 54 | 51.9% | 0.567 |
| T | 18 | 42.9% | 50 | 48.1% | ||
| AGTT174M | T | 37 | 88.1% | 93 | 89.4% | 0.816 |
| M | 5 | 11.9% | 11 | 10.6% | ||
| ACEI/D | I | 15 | 35.7% | 41 | 39.4% | 0.677 |
| D | 27 | 64.3% | 63 | 60.6% | ||
| AGTM235T | M | 44 | 53.7% | 34 | 53.1% | 0.949 |
| T | 38 | 46.3% | 30 | 46.9% | ||
| AGTT174M | T | 72 | 87.8% | 58 | 90.6% | 0.588 |
| M | 10 | 12.2% | 6 | 9.4% | ||
| ACEI/D | I | 28 | 34.1% | 28 | 43.8% | 0.236 |
| D | 54 | 65.9% | 36 | 56.3% | ||
| Blood pressure (optimal) | ||||||
| Normal | Optimal | |||||
| Count | Column N % | Count | Column N % | |||
| AGTM235T | M | 65 | 55.1% | 13 | 46.4% | 0.409 |
| T | 53 | 44.9% | 15 | 53.6% | ||
| AGTT174M | T | 106 | 89.8% | 24 | 85.7% | 0.738 |
| M | 12 | 10.2% | 4 | 14.3% | ||
| ACEI/D | I | 45 | 38.1% | 11 | 39.3% | 0.910 |
| D | 73 | 61.9% | 17 | 60.7% | ||
Grade 1 hypertension (140-159 and/or 90-99 mmHg), High normal (130-139 and/or 85-89 mmHg), Normal (120-129 and/or 80-84 mmHg) and Optimal (<120/<80 mmHg).
Abbreviations: AGT: Angiotensinogen; ACE: Angiotensin-1-converting enzyme
Genotype and alleles in association with blood pressure differences changes.
| Systolic Blood Pressure | Diastolic Blood Pressure | ||||||
|---|---|---|---|---|---|---|---|
| (Changes in mmHg) | (Changes in mmHg) | ||||||
| Mean | Standard Deviation | p | Mean | Standard Deviation | p | ||
| AGTM235T | MM | -22.9 | 26.1 | 0.282 | -8.4 | 12.7 | 0.521 |
| MT | -32.6 | 20.6 | -12.2 | 11.7 | |||
| TT | -31.9 | 20.4 | -11.3 | 11.0 | |||
| AGTT174M | TT | -29.8 | 22.9 | 0.977 | -10.9 | 12.0 | 0.909 |
| TM | -30.0 | 20.3 | -11.3 | 11.4 | |||
| MM | 0.0 | 0.0 | 0.0 | 0.0 | |||
| ACEI/D | II | -20.0 | 31.8 | 0.282 | -6.1 | 14.5 | 0.409 |
| ID | -32.9 | 22.0 | -11.9 | 11.1 | |||
| D | -28.7 | 17.8 | -11.4 | 11.9 | |||
| Systolic blood pressure | Diastolic blood pressure | ||||||
| Mean | Standard Deviation | p | Mean | Standard Deviation | p | ||
| AGTM235T allele | M | -27.7 | 23.7 | 0.216 | -10.3 | 12.2 | 0.449 |
| T | -32.3 | 20.2 | -11.8 | 11.2 | |||
| AGTT174M allele | T | -29.8 | 22.4 | 0.979 | -11.0 | 11.8 | 0.915 |
| M | -30.0 | 20.3 | -11.3 | 11.4 | |||
| ACEI/D allele | I | -28.8 | 25.6 | 0.637 | -10.1 | 12.3 | 0.442 |
| D | -30.6 | 19.7 | -11.6 | 11.4 | |||
Abbreviations: AGT: Angiotensinogen; ACE: Angiotensin-1-converting enzyme.
The oligonucleotide primers used for AGTT174M (rs4762) polymorphism were 5’-CAGGGCTGATAGCCAG GCCCA-3’ and 5’-GAGAGCCAGGCCCTGCACAAA−3. PCR was subjected to 95 οC for 5 min, thirty five cycles of 95οC for 30 s, 64οC for 30 s and 72οC for 30 s and final extension to 72οC for 7 min, producing a fragment of 103 bp. This fragment was subsequently cleaved by restriction enzyme NcoI (Nocardia coralline), creating fragments for M allele 70 bp and 33 bp and for T allele 103 bp, which were subjected to electrophoresis on an agarose gel 4% and visualized with ethidium bromide (Fig. 2).
The polymorphism ACEI/D (rs1799752) within the ACE gene was analyzed as previously described [6]. The PCR product is a fragment of 190 bp when the insertion is absent and 490 bp when the insertion is present analyzed by electrophoresis on a 4% agarose gel stained with ethidium bromide.
STATISTICAL ANALYSIS
All continuous variables are presented as mean ± standard deviation while the categorical ones as absolute (N) and relative (percentage) frequencies. Independent samples t-test was used to investigate for any differences of the continuous variables between the two study groups, while paired samples t-test was used in order to evaluate the differences in BP variables between baseline and after treatment. Pearson’s chi-square or Fisher’s exact statistic were used for testing of potential associations between categorical variables. Univariate logistic regression models were constructed in order to quantify any significant association that could derive from the simple associations. All tests were two-sided at a significance level of p<0.05. Data were analyzed using STATA™ (Version 13.0, Stata Corporation, College Station, TX 77845, USA).
RESULTS
There were no failures in sample collection, DNA acquisition or genotyping procedures.
CLINICAL AND LABORATORY PARAMETERS
Demographic data, clinical characteristics and lipid profile of the study groups are shown in Table 1. By definition of the study protocol the prevalence of coronary artery disease, stroke and diabetes mellitus was presented in the hypertensive group only (28.9, 4.8 and 27.7%, respectively). Furthermore 12% were current smokers compared with the Control group where smokers were nearly 3 times higher, p=0.001. Age, body mass index (BMI), total cholesterol (TC), triglycerides (TGs) and low-density lipoprotein cholesterol (LDL-C) were significantly lower in the Control group compared with the hypertensive group (p=0.01 for all comparisons).
GENE FREQUENCY AND HYPERTENSION
Genotype frequencies are shown in Table 2. The genotype and allele distribution of the AGTM235T variant significantly differed between hypertensives and normotensives odds ratio (OR) = 1.57% (T vs M allele), 95% confidence intervals (CIs): 1.01 - 2.44; p = 0.045 for hypertensives in the ramipril group. Specifically, the hypertensive group had more frequently the TT genotype compared with normotensive controls, p=0.042, Table 2. However, neither the aforementioned association nor any other cross-tabulation between genotype and allele distribution and study group were significant when tested by gender.
GENE POLYMORPHISMS AND RAMIPRIL TREATMENT
None of the 3 studied SNPs were associated with the BP-lowering response to ramipril (Tables 3-5). Genotype and allele frequencies of AGTM235T, AGTT174M and ACEI/D gene polymorphisms were evaluated according to BP-lowering response define as Grade 1 hypertension (140-159 and/or 90-99 mmHg), High normal (130-139 and/or 85-89 mmHg), Normal (120-129 and/or 80-84 mmHg) and Optimal (<120/<80 mmHg).
DISCUSSION
As there is a genetic predisposition to hypertension and elevated BP is inadequately controlled, several candidate genes have been investigated with regard to BP regulation. AGT and ACE genes that affect the RAS have been widely evaluated [6, 7]. In the present study, we evaluated 3 SNPs in 2 candidate genes involved in RAS-related pathways, also investigating their potential impact on ramipril monotherapy efficacy. We found that AGTM253T (rs699) gene polymorphism frequency is different between hypertensives and controls. No differences in the frequency of AGTT174M (rs4762) and ACEI/D (rs1799752) gene polymorphisms between the 2 study groups were observed. Furthermore, none of these 3 SNPs was shown to affect the BP-lowering effects of ramipril monotherapy.
Jeunemaitre et al. [9] originally explored the potential role of AGT gene in hypertension through a linkage study. Two different meta-analyses in Chinese populations confirmed that the T allele of AGTM235T polymorphism is associated with essential hypertension [19, 20]. However, Niu et al found no association of essential hypertension with AGTM235T or AGTT174M polymorphisms, even after stratification by age, gender or disease severity [21]. Similarly, Caulfield et al. [22] did not report any association with either AGTM235T or AGTT174M gene polymorphisms. Mohana et al. [23] reported an increase in the risk for hypertension in women only with the AGTM235T polymorphism (OR = 2.82; 95% CI = 1.22-6.49; p=0.012). Therefore, some studies confirm the association [11, 24] and others refute it [25-27]. In our study, the hypertensive group had approximately 3 times more frequently the TT genotype of the AGTM235T gene polymorphism compared with normotensive controls, p=0.042.
With regard to the AGTT174M polymorphism, Mohana et al. [23] reported significant differences between hypertensives and normotensives. Also, a meta-analysis of the association of 4 AGT polymorphisms with essential hypertension confirmed this association [28]. Although an analysis by ancestry revealed that in Asian and mixed populations the 174M allele was associated with an increased risk for hypertension (OR: 1.31; 95% CI: 1.02 - 1.69; p = 0.04 and OR: 1.43; 95% CI: 1.11 - 1.83; p = 0.005, respectively), no clear evidence for a role of this variant is observed in European ethnicity populations (OR: 1.03; 95% CI: 0.92 - 1.15; p = 0.61) [25]. In our study, we did not find any differences in the frequency of this polymorphism between the 2 study groups.
With regard to ACEI/D gene polymorphisms, there are studies with inconsistent results. Dhanachandra Singh Kh et al. [29] found overrepresentation of the ACE I allele in normotensive males, thus suggesting its protective role. He et al. [13] also found that the ACEI/D gene polymorphism plays a role in hypertension. Furthermore, meta-analyses reported that DD genotype of the ACEI/D polymorphism [14] were associated with essential hypertension. In the present study, we did not observe any differences in ACEI/D gene polymorphism frequency between the 2 study groups. Similarly, no association was found in Chinese, Italian, Greek, Japan and Indian populations [30, 31]. Whether this disagreement is due to racial, environmental factors or the inclusion criteria used in each study is unknown and needs additional investigation.
There are only a few studies evaluating the association between AGTM235T, AGTT174M and ACEI/D gene polymorphisms with the BP-lowering effect of ramipril. Zivko et al. [32] did not find any significant impact of ACEI/D gene polymorphisms on ramipril-related BP-decreasing effect in 66 hypertensive patients. Similarly, in the present study, we did not observe any significant differences in BP changes with regard to I/D polymorphism. In contrast, Gupta et al. [33] reported that the percentage of responders to ramipril therapy was significantly higher in patients with the II genotype compared with those with the ID genotype. As there is an inconsistency of findings across studies, the effects of these polymorphisms on ramipril-related BP changes still remain unclear.
With regard to the other 2 AGT SNPs (M235T and T174M), to our knowledge, the present study is the first to evaluate their association with ramipril efficacy, reporting no correlations. It should be noted that the main limitation of this study is the relatively small sample size.
CONCLUSION
In the present study, we found that only the frequency of AGTM235T (rs699) variant is significantly (p=0.045) different between hypertensives and controls. No gender differences in the frequency of AGTT174M (rs4762),
AGTM235T (rs1799752) and ACEI/D (rs1799752) gene polymorphisms were observed in both study groups. Furthermore, these 3 SNPs did not influence the BP-lowering efficacy of ramipril. However, as this is a small study, future research on larger populations is needed to establish these associations.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

