All published articles of this journal are available on ScienceDirect.

Low Vitamin D and Cardiovascular Risk Factors in Males and Females from a Sunny, Rich Country
Authors Info & Affiliations
Abstract
Background:
Low serum vitamin (vit) D levels are common even in sunny countries. We assessed the prevalence and relationship of low vit D with cardiovascular risk factors in Qatar.
Methods:
Data were collected retrospectively from January 2008 and November 2009. In patients who had low vi t D (< 30 ng/ml ) , demographic and clinical profiles were analyzed and compared in males and females.
Results:
The overall mean level of vit D among 547 patients was 14.4±11 ng/mL. Among the low vitamin D group, 56% were females (mean age 48±12) and 44% males (mean age 49.6±13). Severely low vit D levels (<10 ng/mL) were found in 231 (46%) patients with mean age of 46±12 years. Compared with females, males with low vitamin D were more likely to have diabetes mellitus (38 vs 22%, p=0.001), dyslipidemia (41 vs 29%, p=0.007), myocardial infarction (5.5 vs 1.5%, p=0.001) and angiographically documented coronary artery disease (CAD) (53 vs 17%, p=0.001). Multivariate logistic regression analysis showed that in the presence of low vit D, age and hypertension were independent predictors of CAD (OR 1.07;95% CI: 1.02-1.11) and OR 8.0; 95% CI: 1.67-39.82), respectively.
Conclusions:
Our study supports the widespread prevalence of low vit D in sunny regions. Low vit D is associated with 3 times increase in the rate of MI among males. Hypertension increases the risk of CAD 8 times in the presence of low vit D regardless of gender.
INTRODUCTION
Insufficient serum vitamin (vit) D level (< 30 ng/ml or < 75 nmol/L) is a common problem worldwide [1-3]. Although sun exposure is the major source of vit D, several reports show that low vit D is common in sunny regions [4-7]. Despite the sunshine, Middle Eastern populations showed a high rate of low vit D due to limited sun exposure based on cultural practices [8-10]. The mean 25(OH)D levels are near 25 nmol/L in Lebanese, Saudi, Emirati, and Iranian females [10-13]. In the elderly Lebanese, 37% of males and 56% of females had vit D levels < 25 nmol/L [10]. Similarly, in an international study conducted in females with osteoporosis, the highest proportion of low vit D was noted in the Middle East [14]. A large proportion of adolescent girls, up to 70% in Iran and 80% in Saudi Arabia had 25(OH)D levels < 25 nmol/L [15,16].
Insufficient vit D affects both males and females in all age groups; however, there is evidence that females have lower levels than males in elderly Europeans [17-19], young adolescents in Lebanon [20], and in a yearly study of the healthy aged in New Zealand [21]. This gender differences may reduce with age [3,22].
Epidemiologic studies have recently linked low vit D with increased risk of cardiovascular events [23]. This association between low vit D level and cardiovascular disease (CVD) has never been explored in our population despite the highly prevalent low vit D. Therefore, we explored the relationship between low Vit D and vascular risk factors in both sexes in Qatar.
METHODS
This is a retrospective, observational study that was conducted at Hamad General Hospital (HGH), Qatar. This hospital provides inpatient and outpatient tertiary care in medicine and surgery for the residents of Qatar (nationals and expatriates) making it an ideal center for population-based studies. Vit D samples were selected randomly from the central laboratory at HGH regardless of the clinic type, indication and whether patients were on vit D supplements.
This was based on the previous evidence of a high prevalence of vit D among people living in the Gulf countries [8-13]. Inclusion criteria were males and females aged between 30 and 60 years living in Qatar. Samples from pediatric, geriatric, and oncology units were excluded. Vit D deficiency was defined as level < 30 ng/ml; subdivided into mild (20-29 ng/ml) moderate (10-19 ng/ml); and severe (<10 ng/ml). Coronary artery disease (CAD) is defined as documented myocardial infarction (MI), angiographically proven CAD or chronic stable angina. Diagnosis of the different types of CAD and definitions of data variables were based on the American College of Cardiology (ACC) clinical data standards [24]. The presence of diabetes mellitus (DM) was determined by the previous or current medical record of a documented diagnosis of DM that had been on treatment (either oral antidiabetic agents or insulin injection). The presence of dyslipidemia was determined by the demonstration of a fasting cholesterol > 5.2 mmol/L in the patient’s medical record, or any history of treatment of dyslipidemia. The presence of hypertension (HTN) was determined by any documentation in the medical record of HTN. Smoking history: patients were divided into current cigarette smokers, past smokers (defined as more than 6 months abstinence from smoking) and those who never smoked.
For measurement of vit D, we used an immunoanalyser (Liaison, Diasorin Inc). It is an automated direct competitive chemiluminescence immunoassay (CLIA) for quantitative determination of total 25-OH vit D in serum or plasma. The imprecision at 56 and 19 ng/l as measured by coefficient of variation was 8.7 and 13.2%, respectively.
Ethical clearance was obtained from the MRC Research Committee, HMC, for the analysis and publication of this study (IRB #9090/09).
Statistical analysis
Data were presented as proportions or mean ± standard deviation (SD) as appropriate. Baseline demographic characteristics, past medical history, clinical presentation, and clinical outcomes were compared between the 2 groups (males and females) using the student-t test for continuous variables and Pearson chi-square (X2) test for categorical variables. Logistic regression analysis for the predictors of CAD in low vit D patients was performed after adjustment for baseline variables [age, sex, DM, obesity, cholesterol and HTN]. A 2-tailed P < 0.05 was considered significant. Data analysis was carried out using the Statistical Package for Social Sciences version 18 (SPSS Inc. USA).
RESULTS
We evaluated 2000 randomly selected blood samples for vit D level between January 2008 and November 2009. Of those samples, 547 fulfilled the inclusion criteria. The overall mean age and level of vit D were 49 ± 13 years and 14.4 ± 11 ng/mL, respectively. There were 498 patients (91%) with a low vit D level (< 30 ng/ml) with mean age of 49 ± 12 years whereas 49 patients (9%) had normal vit D level (30 - 80 ng/ml) with mean age of 54 ± 13 years. In patients with low vit D, severely low levels (<10 ng/ml) were found in 231 (46%) patients with mean age of 46 ± 12 years. Fig. (1) shows a trend of steadily rising vit D levels with increasing age. The number of females and males stratified according to vit D levels are shown in Fig. (F2). In all categories of vit D levels, the numbers of females were greater compared with males.
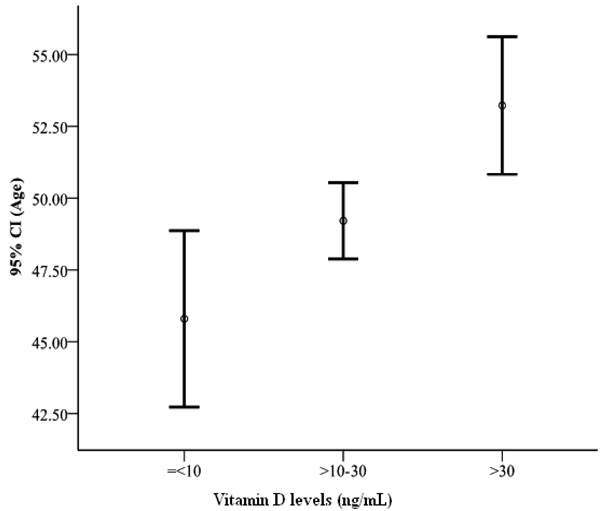
Vitamin D levels according to age.

Number of males and females stratified by vitamin D levels.
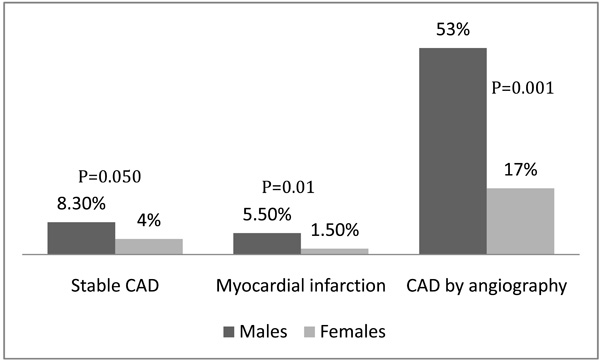
Shows the prevalence of coronary artery disease among males and females who had low vitamin D levels.
Low Vitamin D (<30 ng/mL)
Among low vit D group, 56% were females, 65% were obese, 38% had HTN, 34% had dyslipidemia and 29% had DM. CAD was diagnosed by previous history of stable angina (6%), history of MI ( 3.3%) or by coronary angiography (27%). Compared with females, males with low vit D were more likely to have DM (38 vs 22%, p = 0.001), dyslipidemia (41 vs 29%, p = 0.007), CAD diagnosed by coronary angiography (53 vs 17%, p = 0.001) and lower left ventricular ejection fraction (14 vs 10%,p = 0.01). Males were likely to have higher serum cholesterol and low-density lipoprotein (P = 0.03 and 0.003, respectively) compared with females (Table 1). Fig. (3) shows the prevalence of CAD among males and females who had low vit D levels.
Demographic Profile and Clinical Characteristics of Patients with Low Vitamin D Levels
| Males | Females | P | |
|---|---|---|---|
| Number | 221(44%) | 277(56%) | |
| Age (mean, years) | 50±13 | 48±12 | 0.23 |
| Diabetes mellitus | 38% | 22% | 0.001 |
| Hypertension | 43% | 35% | 0.052 |
| Smoking | 7% | 9% | 0.73 |
| Dyslipidemia | 41% | 29% | 0.007 |
| Obesity | 65% | 60% | 0.31 |
| Cerebrovascular disease | 1.8% | 1.5% | 0.76 |
| Chronic renal failure | 1.8% | 3.3% | 0.31 |
| Low LV Ejection Fraction (<50%) | 14% | 10% | 0.001 |
| On statin | 29% | 22% | 0.06 |
| On aspirin | 23% | 15% | 0.03 |
| Hemoglobin A1c (%) | 6.6±2 | 6.4±1.7 | 0.29 |
| Hemoglobin (g/dl) | 12.3±12 | 12.3±2 | 0.64 |
| Cholesterol (mmol/L) | 5.2±1.1 | 4.9±1.2 | 0.03 |
| Triglycerides (mmol/L) | 1.8±2 | 1.5±0.8 | 0.07 |
| Low Density Lipoprotein (mmol/L) | 3.2±1.04 | 2.9±0.93 | 0.003 |
| High Density Lipoprotein (mmol/L) | 1.30±0.8 | 1.31±0.4 | 0.73 |
| Mean vitamin D (ng/ml) | 11.9±7.4 | 11.9±7.5 | 0.91 |
| Parathyroid hormone values (pg/ml) | 54±42 | 54±40 | 0.97 |
*= creatinine >1.5 upper normal range (124 mmol/L).
Predictors for Coronary Artery Disease in Patients with Low Vitamin D (<30 ng/ml).
| Univariate Analysis* | Multivariate Analysis* | |
|---|---|---|
| Age | 1.11(1.07-1.15), P=0.001 | 1.07(1.02-1.11), P=0.002 |
| Sex | 0.51(0.22-0.99), P=0.050 | 0.63(0.26-1.47), P=0.28 |
| Diabetes mellitus | 5.7(2.59-12.43), P=0.001 | 1.32(0.53-3.33),P=0.55 |
| Obesity | 1.13(0.53-2.43), P=0.75 | 0.75(0.31-1.77), P=0.51 |
| Hypertension | 26(6.26-112.50), P=0.001 | 8.14(1.67-39.82), P=0.01 |
| Dyslipidemia | 4.6(2.12-10.12), P=0.001 | 1.08(0.44-2.66), P=0.87 |
* = odds ratio(95% confidence interval)
Table 2 demonstrates the predictors of CAD in the presence of low vit D (< 30 ng/ml). Multivariate logistic regression analysis showed that in the presence of low vit D, age and hypertension were independent predictors of CAD (OR 1.07; 95% CI:1.02-1.11) and OR 8.0; 95% CI:1.67-39.82), respectively.
DISCUSSION
The present study demonstrates the prevalence and impact of low vit D in males and females in a sunny country. Our key findings were: 1) High prevalence of low vit D in Qatar. In the last few years, measuring the serum level of vit D is routine in most of rheumatology, general internal medicine, cardiology, geriatric, oncology and nephrology out-patient clinics. This practice was based on the high prevalence of low vit D in countries similar to Qatar in regard with traditional, cultural and environment characteristics [8-13] 2) Low vit D is significantly associated with high prevalence of DM, dyslipidemia (high total cholesterol and LDL) and CAD in males compared with females. 3) The trend for low vit D levels fell with age. 4) Low vit D is associated with 3 times increase in the rate of MI among males. 5) HTN increases the risk of CAD 8 times in the presence of low vit D regardless of gender.
After discovery of oil, the life style in the Arab Gulf region including Qatar have become progressively more modernized based on technology, sedentary activity, and unhealthy dietary patterns [25]. These factors have led to a higher prevalence of low vit D despite of the presence of sun most of the year. Vit D deficiency is well recognized in Middle Eastern females as a result of cultural habit of remaining covered, while vit D level among males in this region remains under-reported. A recent study reported that 25(OH)D deficiency is common among otherwise healthy Middle Eastern male athletes [26]. Assessment of vit D deficiency among health care professionals working at HGH in Qatar showed the overall mean of vit D level was 11.7 ng/ml. It was lower in females (10.3 ng/ml) than in males (13.7 ng/ml) and 97% of all participants had a mean level <30 ng/ml [27]. Furthermore, a recent study among Qatar university students showed that 53.5% of Qatari females of college age had severe vit D deficiency and 43.6% have insufficient levels of vit D [28] Low vit D predisposes to hypertension, DM, metabolic syndrome, heart failure and stroke [1,29-35]. A study of male health professionals showed a 2-fold risk of MI in subjects who were vit D deficient compared with those in the normal range [36]. The mechanism by which vit D may affect the cardiovascular system includes effects on vascular smooth muscle proliferation, inflammation and vascular calcification. Vit D deficiency activates the renin-angiotensin system leading to HTN and left ventricular hypertrophy [37-39]. However, the association between vit D status and CVD is not well-defined. Epidemiologic evidence and observational studies showed potential benefits of vit D [37]. Prospective studies demonstrated that low levels of vit D precede the development of CVD [40]. A follow-up study based on Health Professionals showed that males with vit D deficiency (15 ng/mL had a twofold increased risk of MI, compared with those with sufficient levels of at least 30 ng/mL. Furthermore, other reports demonstrated that vit D deficiency may increase CVD risk, irrespective of established risk factors for CVD [41, 42].
The high prevalence of vit D deficiency in sunny cities especially among females and younger population emphasizes the need for a recommendation to monitor 25(OH)D, modify life style and nutritional habits [43-45].
Limitations of the current study included retrospective nature and lack of detailed treatment information. Data were collected randomly from the central Lab records without determination of the treatment of patients or the type of subspecialty.
CONCLUSIONS
Our study substantiates the evidence of a widespread prevalence of low vit D in the sunny regions. HTN is associated with 8 times increased the risk of CAD in the presence of low vit D regardless of gender. Therefore, screening and treatment of low vit D may be important in hypertensive patients, particularly since some evidence showed that vit D sufficiency lowers the blood pressure in hypertensive patients [46]. Low vit D is associated with 3 times increase in the rate of MI among males. However, as reports from randomized controlled trials the association between vit D and CVS are limited. There is a need for such studies in our region.
CONFLICT OF INTEREST
None declared.
ACKNOWLEDGEMENT
We thank laboratory staff of Hamad General Hospital for the technical support. The authors have no financial issues to disclose.

