All published articles of this journal are available on ScienceDirect.

Effects of Thyroid Dysfunction on Lipid Profile
Abstract
Thyroid dysfunction has a great impact on lipids as well as a number of other cardiovascular risk factors. Hypothyroidism is relatively common and is associated with an unfavorable effect on lipids. Substitution therapy is beneficial for patients with overt hypothyroidism, improving lipid profile. However, whether subclinical hypothyroidism should be treated or not is a matter of debate. On the other hand, hyperthyroidism can be associated with acquired hypocholesterolemia or unexplained improvement of lipid profile. Overall, thyroid dysfunction should be taken into account when evaluating and treating dyslipidemic patients.
1. INTRODUCTION
Thyroid function regulates a wide array of metabolic parameters. Thyroid function significantly affects lipoprotein metabolism as well as some cardiovascular disease (CVD) risk factors, thus influencing overall CDV risk [1-3]. Indeed, even within the normal range of thyroid-stimulating hormone (TSH) values, a linear increase in total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C) and triglycerides (TGs) and a linear decrease in high-density lipoprotein cholesterol (HDL-C) levels has been observed with increasing TSH [4].
2. MECHANISMS (FIG. 1)
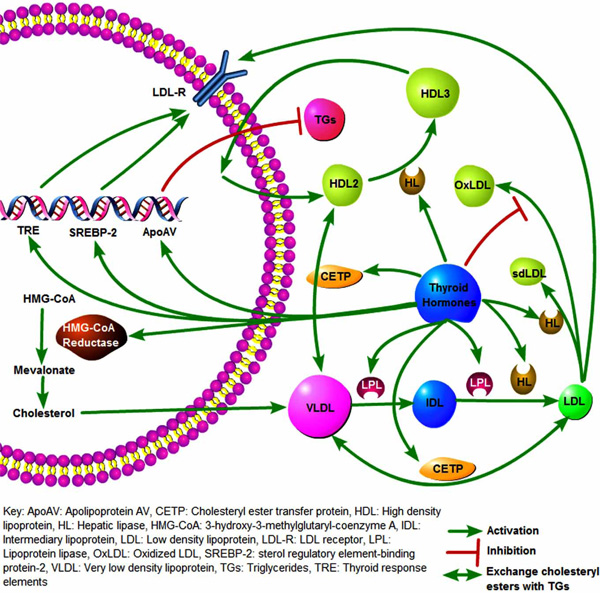
Effects of thyroid hormones on lipid metabolism.
Thyroid hormones induce the 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase, which is the first step in cholesterol biosynthesis. Moreover, triiodothyronine (T3) upregulates LDL receptors by controlling the LDL receptor gene activation. This T3-mediated gene activation is done by the direct binding of T3 to specific thyroid hormone responsive elements (TREs) [5]. Furthermore, T3 controls the sterol regulatory element-binding protein-2 (SREBP-2), which in turn regulates LDL receptor’s gene expression [6]. T3 has also been associated with protecting LDL from oxidation [7].
Thyroid hormones can influence HDL metabolism by increasing cholesteryl ester transfer protein (CETP) activity, which exchanges cholesteryl esters from HDL2 to the very low density lipoproteins (VLDL) and TGs to the opposite direction [8]. In addition, thyroid hormones stimulate the lipoprotein lipase (LPL), which catabolizes the TG-rich lipoproteins, and the hepatic lipase (HL), which hydrolyzes HDL2 to HDL3 and contributes to the conversion of intermediate-density lipoproteins (IDL) to LDL and in turn LDL to small dense LDL (sdLDL) [9, 10]. Another effect of T3 is the up-regulation of apolipoprotein AV (ApoAV), which plays a major role in TG regulation [11]. Indeed, increased levels of ApoAV have been associated with decreased levels of TGs [12]. Proposed mechanisms for this effect include the decrease of hepatic VLDL-TG production and the increase of plasma LPL levels and activity, resulting in increase of lipoprotein remnant generation due to enhanced LPL-mediated lipolysis of VLDL-TG [12]. Moreover, a greater clearance of lipoprotein core remnants, caused by increased hepatic uptake due to an enhanced affinity for the LDL receptor, has also been ascribed to ApoAV [12].
Beyond their effect on lipid profile thyroid hormones can equally affect a number of other metabolic parameters related to CVD risk. Indeed, thyroid function can influence adipocyte metabolism and the production of adipokines [13-15]. Hyperthyroidism has been associated with increased levels of adiponectin, whereas hypothyroidism is not associated with significant changes in adiponectin [13, 15]. Insulin resistance is also correlated with thyroid function [16-19]. TSH is positively associated with fasting and postprandial insulin concentration and negatively with insulin sensitivity [17]. Moreover, low normal FT4 levels are significantly associated with increased insulin resistance [19]. Oxidative stress is also affected by thyroid function with studies however showing controversial outcomes [7, 20]. Furthermore, endothelial [17] and cardiac function as well as atherosclerosis [21] have been positively associated with thyroid hormone levels. A positive association between TSH and body mass index (BMI) or waist circumference has also been described [22, 23]. A large population trial using data from the fourth and fifth Tromso study showed that this association between TSH and BMI was only significant in non smokers [24].
The effects of thyroid dysfunction on lipid parameters and CVD risk factors as well as the influence of substitution therapy are discussed below.
3. HYPOTHYROIDISM
Hypothyroidism is a common metabolic disorder in the general population. Indeed, data from the third National Health and Nutrition Examination Survey (NHANES III) showed a 4.6% prevalence of hypothyroidism in the general population, while 9.5% of the Colorado prevalence study participants had elevated levels of TSH [3]. Thyroid failure is more common in women and its prevalence rises with age. Hypothyroid patients have increased levels of TC and LDL-C [3]. Indeed, hypothyroidism is a common cause of secondary dyslipidemia [25, 26].
i. Overt Hypothyroidism
a. Lipid Profile
Although decreased thyroid function is accompanied by reduced activity of HMG-CoA reductase, TC and LDL-C levels are increased in patients with overt hypothyroidism [27-31]. This is due to the decreased LDL-receptors’ activity, resulting in decreased catabolism of LDL and IDL [32-34]. Moreover, a decrease in LPL activity is found in overt hypothyroidism, decreasing the clearance of TG-rich lipoproteins [35]. Therefore, overt hypothyroid patients may also present with elevated TG levels associated with increased levels of VLDL and occasionally fasting chylomicronemia [29-31, 34]. The VLDL and IDL particles in hypothyroidism are rich in cholesterol and apolipoprotein E, thus resembling β-VLDL particles of type III hyperlipoproteinemia. Therefore, the full-blown clinical syndrome of the type III hyperlipoproteinemia may develop in patients homozygous for the apolipoprotein E2 allele if they become hypothyroid.
Hypothyroid patients may also exhibit elevated levels of HDL-C [27] mainly due to increased concentration of HDL2 particles. Indeed, due to a reduction of HL activity a decrease in HDL2 catabolism is observed. [36]. Moreover, decreased activity of the CETP results in reduced transfer of cholesteryl esters from HDL to VLDL, thus increasing HDL-C levels [37]. Hypothyroid patients have increased lipoprotein (a) [Lp(a)] levels [38, 39], which are associated with increased CVD risk [39, 40].
Beyond the levels of LDL-C, the qualitative composition of LDL-C plays an important role in CVD development. Indeed, increased sdLDL concentration increases the risk for CVD [41]. Trials evaluating the effects of overt hypothyroidism on LDL subfractions have shown conflicting results. A study in newly-diagnosed hypothyroid patients (n=60) showed that hypothyroidism was associated with higher prevalence of sdLDL [28]. On the other hand, there have been studies showing no significant differences between overt hypothyroid patients and healthy controls regarding sdLDL levels [42, 43]. Another study evaluated the effects of short-term overt hypothyroidism on LDL subfractions [27]. Thyroidectomized patients (n=28) were withdrawn from substitution therapy for 2-3 weeks in preparation for radioactive iodine ablation. Patients exhibited an increase in LDL-C that was found to be primarily due to increases in the large LDL particles, while sdLDL did not significantly change [27].
b. CVD Risk
The above abnormalities of lipid metabolism associated with overt hypothyroidism predispose to the development of atherosclerotic coronary artery disease (CAD) [44, 45]. Moreover, hypothyroidism can adversely affect other CVD risk factors, further contributing to increasing CAD risk. Decreased thyroid function not only increases the number of LDL particles, but also promotes LDL oxidability [46]. Furthermore, hypothyroidism increases plasma homocysteine levels [47-50], which can be attributed to the hypothyroidism-induced decline of kidney function [51] as well as impaired methylenetetrahydrofolate reductase activity [52]. In addition, thyroid failure is strongly associated with arterial hypertension (especially diastolic) [53-55] via sympathetic and adrenal activation [53], and increased vascular stiffness [54, 56, 57]. Subjects with overt hypothyroidism also exhibit impaired endothelial function [58], increased uric acid [28] and phosphate levels [29], all of which are associated with increased CVD risk [59, 60].
In addition, an increase in carotid intima media thickness (CIMT) has been observed in hypothyroid patients [61]. Hypothyroidism is also accompanied by increased prevalence of metabolic syndrome [62] and waist-to-hip ratio [63]. Insulin resistance is increased in thyroid failure [64], while a decrease in GLUT4 glucose transporters (leading to a reduction of glucose uptake and promoting insulin resistance [65]) is observed [64]. Moreover, there are indications of increased high-sensitivity C-reactive protein (hsCRP) levels in hypothyroidism [28, 49] although there are studies which do not support this notion [31, 50].
c. Substitution Therapy
Administration of substitution therapy with L-thyroxine significantly improves lipid metabolism abnormalities. A period of 4-6 weeks of thyroxin replacement therapy is usually needed to correct dyslipidemia in overt hypothyroidism. In general, changes in serum lipoproteins in hypothyroid patients are correlated with changes in free T4 (FT4) [66]. A study in newly-diagnosed hypothyroid patients (n=60) showed a decrease in serum TC and LDL-C levels after thyroxine treatment [28]. However, when the effects of substitution therapy on qualitative lipid profile were assessed no change in LDL particle size was seen [28]. A more dramatic reduction of TC levels has been observed in hypothyroid patients with higher baseline TSH levels [67].
Serum HDL-C levels tend to decrease with thyroid replacement, but this is a less consistent finding [68]. Serum Lp(a) levels also tend to decrease with restoration of euthyroidism [25, 39]. Moreover, a decrease in CIMT has been observed after thyroxine treatment in hypothyroid patients [61].
The presence of overt hypothyroidism in patients with dyslipidemia is not rare. We found that 2.8% of the patients who visited our outpatient lipid clinic with dyslipidemia had elevated levels of TSH and reduced levels of FT4 [25]. After restoration of euthyroidism with levothyroxine therapy, a significant decrease of serum levels of TC and LDL-C, apolipoprotein B (ApoB) and Lp(a) was observed, while levels of HDL-C, TGs and apolipoprotein AI (ApoAI) were not significantly changed [25]. Superimposed dyslipidemia should be taken into account in cases of failure of substitution therapy to normalize the lipid profile despite the restoration of euthyroidism [1].
Hypothyroidism is one of the most common causes of secondary dyslipidemia. Therefore, before starting hypolipidemic therapy, the evaluation of thyroid function is needed. Thyroid failure is associated with increased levels of creatinine kinase (CK) [69]. Statin therapy may substantially increase levels of CK. A study examined the effects of accidentally starting statin therapy in patients with undiagnosed hypothyroidism (n=9) [70]. These patients had significantly higher CK levels (1095 U/L) compared with untreated hypothyroid patients matched for freeT4 levels (n=18; CK=395; p<0.05) [70]. Therefore, it is imperative to firstly correct thyroid dysfunction with thyroxine substitution therapy and then treat the underlying dyslipidemia with statins.
ii. Subclinical Hypothyroidism
Subclinical hypothyroidism (SH), defined as the clinical status of elevated serum TSH levels with normal levels of FT4 and FT3, is a far more common disorder than overt hypothyroidism. The prevalence of SH in the general population is estimated at 4.3% - 9% [3, 71]. SH has a higher prevalence among women and older populations [3, 72-74]. Moreover, SH may progress to overt hypothyroidism. The rate of progression is higher with the concomitant presence of thyroperoxidase antibodies (TPO-Ab) or higher levels of TSH [75].
a. Lipid Profile
SH is associated with increased levels of TC and LDL-C [63, 72, 74, 76-80]. In addition, some studies have shown that SH dyslipidemia may also be accompanied by increased TGs [81, 82] and decreased HDL-C levels [83]. Moreover, subjects with high normal TSH levels (2-4 mIU/L), but with positive antithyroid antibodies may also exhibit elevated cholesterol levels [84]. In a cross-sectional study we evaluated serum lipid parameters of SH patients (n=66) and age- and sex- matched euthyroid controls (n=75) [85]. Patients with SH had significantly higher levels of TC, LDL-C and ApoB, whereas levels of TGs, HDL-C and ApoAI did not differ significantly compared with euthyroid controls [85]. Similarly, results from the fifth Tromso Study showed increased levels of LDL-C in SH patients (n=84) [86].
Most studies have shown increased Lp(a) levels related to SH [85, 87, 88]. An interesting study evaluated serum Lp(a) levels along with corresponding apolipoprotein(a) [apo(a)] phenotypes, which are known to influence Lp(a) levels, in SH patients [89]. SH patients had higher Lp(a) levels compared with controls (p=0.003). Of note, no significant difference in the frequencies of apo(a) phenotypes were detected between patients with SH (n=69) and controls (n=83).
Thyroid autoimmunity may also play an important role in the elevation of Lp(a) levels. It has been reported that euthyroid males and postmenopausal females with evidence of thyroid autoimmunity (increased titers of TPO-Ab and/or thyroglobulin autoantibodies) have increased Lp(a) levels [90]. On the other hand, a study compared the levels of Lp(a) of 22 euthyroid subjects (9 male and 13 postmenopausal female) with thyroid autoimmunity with those of 64 age- and sex-matched controls without thyroid autoimmunity [91]. There were no significant differences in the values of lipid parameters, including Lp(a), between the two groups even when apo(a) phenotypes were taken into account [91]. Moreover, no significant difference in the Lp(a) levels was found in euthyroid patients with chronic renal failure regardless of the presence of thyroid autoimmunity, the apo(a) phenotype, the stage of renal failure and the mode of dialysis in end stage patients [92]. Furthermore, the presence of thyroid autoimmunity has not been shown to influence serum lipid parameters in SH subjects [85].
There is some controversy regarding the presence or the severity of SH-induced dyslipidemia. Indeed, there have been studies indicating no significant difference in lipid profile between SH patients and controls [29-31, 93]. Data from the NHANES III revealed increased levels of TC in SH patients (n=215) vs controls (n=8013) [94]. However, when adjusted for age, race, sex and the use of lipid-lowering drugs no difference was observed between SH and controls regarding lipid profile. Moreover, there have been studies questioning the effects of thyroid hormones on Lp(a) levels. Various studies have shown no difference between SH and control subjects regarding Lp(a) levels [39, 82, 95, 96]. Lee et. al compared patients covering the whole spectrum of thyroid function and found no differences in Lp(a) between groups [31]. Moreover, no correlation was found between Lp(a) levels and TSH or FT4 [31]. On the contrary, in a study with SH patients (n=38) a significant negative correlation (r=-0.31; p=0.03) was observed between FT3 levels and Lp(a) [82].
An association between lipids, thyroid function and insulin resistance has been observed [18]. The analysis of a subgroup from the Fremantle Diabetes Study (FDS) showed that the association of TSH levels and lipid profile is significant mainly in the presence of insulin resistance. Similar results were shown in a study in euthyroid subjects [97].
An interesting aspect of the potential SH-mediated dyslipidemia is the qualitative effects of thyroid hormones on lipids. A study compared SH women (n=21) with female controls (n=11) [93]. No difference was found regarding lipid profile between the 2 groups. However, decreased ratio of cholesterol/triglycerides in LDL (p<0.02) in SH subjects vs controls indicated the presence of more TG-enriched LDL particles in those subjects. On the other hand, a study in SH patients (n=57) did not reveal any differences in LDL particle size compared with controls [42].
b. CVD Risk
Beyond lipids, SH can have a deleterious effect on several other CVD risk factors. SH has been associated with a hypercoagulable state [77, 83]. Furthermore, SH impairs ventricular function as well as cardiovascular and respiratory adaptation to effort and decreases heart rate variability [98, 99]. Moreover, SH decreases flow-mediated vasodilation and nitric oxide (NO) availability, which are markers of endothelial function [98, 99]. An increase in CIMT has also been described in SH patients compared with controls [78, 79]. However, a study in SH patients (n=21) did not confirm such an increase in CIMT compared with euthyroid subjects [100]. Although SH patients with TPO-Ab had higher CIMT values compared with SH patients without TPO-Ab this difference was not significant [100].
A study showed a higher incidence of multi-vessel disease in angina patients (n=344) with high TSH values although TSH was not established as a predictor for coronary artery stenosis [101]. On the other hand, a study in hypothyroid patients (n=794, 90% of whom had SH) did not reveal any differences regarding carotid atherosclerosis (carotid plaques prevalence, severity and CIMT) compared with euthyroid subjects (n=1588) after adjusting for various CVD risk factors [102]. SH has also been associated with other CVD risk factors, such as increase in insulin resistance [64, 103].
SH subjects have been described to have higher plasma lipoprotein-associated phospholipase A2 (Lp-PLA2) (which is a known CVD marker [104]) and lower HDL Lp-PLA2 (which is associated with the antiatherogenic effects of HDL [105]) activity [81]. Moreover, a negative association between free thyroxine and hsCRP levels has been described [106]. Indeed, increased hsCRP levels have been found in SH patients [49]. A study demonstrated a linear correlation between blood pressure and TSH even within the normal reference ranges [107]. However, a large cross-sectional study in SH patients (n=806) did not find any association between SH and increased blood pressure [108]. In addition, smoking may deteriorate the lipid profile in women with SH and aggravate the degree of thyroid failure, thus contributing to the development of atherosclerosis [109].
As described above, SH is positively correlated with increased prevalence of some CVD risk factors. However, it is imperative to investigate the available data on the incidence of CVD morbidity and mortality in SH subjects. A meta-analysis of 14 trials found an increase in risk of CVD (odds ratio [OR] 1.65; 95% CI 1.28-2.12) in subjects with SH [110]. An interesting study evaluated the association of SH with the incidence of congestive heart failure (CHF), CAD, stroke, peripheral artery disease and CVD or total mortality [111]. This was a prospective analysis in a longitudinal cohort study of older adults (aged 70-79 years old) from the Health, Aging, and Body Composition (HEALTH ABC) study. SH subjects (n=338) were subdivided in groups according to their TSH levels. Patients with TSH levels ≥7 mIU/L had a greater risk for CHF (p=0.006). SH was not associated with increased prevalence of stroke, peripheral artery disease and CVD mortality. However, SH subjects with TSH ≥10 mIU/L had a higher risk for myocardial infarction (MI) (hazard ratio [HR] 4.73 95% CI 1.01-22.13) and total mortality (HR 3.13 95% CI 1.11-8.79). Similarly, a recent meta-analysis found a 41% increase in all cause mortality in SH patients compared with euthyroid subjects [112]. Another study in SH patients (n=257) found a positive correlation between SH, CAD and total mortality which however was limited only to men (OR 4; 95% CI 1.4 - 11.5) [113].
Of interest are the results from studies evaluating the effects of SH in elderly populations. The Rotterdam study found an association between SH and aortic atherosclerosis (OR 1.7; 95% CI 1.1 - 2.6) and MI (OR 2.3; 95% CI 1.3 - 4) in elderly SH women [114]. Moreover, the presence of TPO-Ab increased the risk for both aortic atherosclerosis (OR 1.9; 95% CI 1.1 - 3.6) and MI (OR 3.1; 95% CI 1.5 - 6.3). However, the presence of TPO-Ab in total study population was not associated with a history of MI. On the other hand, the Cardiovascular Health Study (CHS) did not find any link between SH and CVD morbidity and mortality in an elderly SH population, although an increased incidence of atrial fibrillation was observed [115]. Moreover, a study evaluated the association of thyrotropin with disability and survival in the Leiden 85-Plus Study elderly population [116]. The results indicated that abnormally high levels of thyrotropin not only did not affect cognitive and mental status but rather prolonged life span [116].
c. Substitution Therapy
A beneficial effect of substitution therapy on lipid parameters and especially TC and LDL-C in some patients with SH has been shown [30, 72, 88, 117-120]. In a meta-analysis, the mean decrease of serum TC and LDL-C levels after thyroxine substitution was -7.9 mg/dL and -10 mg/dL, respectively [72]. The reduction was larger in individuals with higher pretreatment cholesterol levels and in hypothyroid individuals taking suboptimal T4 doses [72]. The fifth Tromso study [86] evaluated the effects of thyroxine (n=32) compared with placebo (n=32) in SH patients. Thyroxine was administered with a goal of TSH levels of 0.5-1.5 mIU/L. The effect of thyroxine therapy on lipid profile was a significant decrease of only ApoB levels (p<0.01). However, when examining the subgroup of patients (n=23) with post-treatment TSH levels 0.2-2 mIU/L a significant decrease in TC (p<0.05) and LDL-C (p<0.01) was also seen. Moreover, thyroxine substitution therapy may have additional advantageous effects to offer beyond the improvement of lipid profile. Indeed, a reduction in CIMT [78, 79] and improvement of endothelial function [99] has been described in SH patients after thyroxine replacement. In addition, thyroxine therapy increased HDL-associated Lp-PLA2 activity in SH subjects [81].
These findings, however, are not consistently corroborated by other studies. Indeed, some studies showed no significant effect of thyroxine therapy on lipid profile in SH patients [78, 93, 121, 122]. Interesting were the results of a study evaluating the effects of thyroxine in SH subjects (n=66) [85]. Lipid profile was not significantly altered with the exception of a decrease in HDL-C levels (p<0.05). However, in the subgroup of patients with TC ≥240 mg/dL (n=14) or TSH ≥10 mIU/L (n=18) a decrease in TC (p<0.05) and LDL-C (p<0.01) was also observed. A recent meta-analysis showed no benefits in survival or CVD mortality after substitution therapy in SH patients [123]. Moreover, thyroxine replacement did not improve quality of life, although a beneficial effect was seen in some lipid parameters and left ventricular function [123].
The beneficial effects of thyroxine substitution therapy on Lp(a) levels in SH subjects are also debated. Several studies have shown no impact of thyroxine therapy on Lp(a) levels in SH patients [39, 40, 85, 88]. However, other studies showed a significant decrease of Lp(a) levels after thyroxine treatment [89, 118]. A study with 17 SH women demonstrated a reduction of Lp(a) by 23.5% (p=0.0005) compared with baseline after substitution therapy [118]. Milionis et al. demonstrated that thyroxine treatment was effective in reducing Lp(a) levels in SH subjects (p=0.008) [89]. Of interest was that this reduction of Lp(a) levels achieved significance only in the low molecular weight apo(a) isoforms subgroup of patients [89].
d. Should we Treat SH Patients?
Although it is clear that thyroid replacement therapy has beneficial effects on serum lipid profile and CVD risk in overt hypothyroid patients, no clear consensus has been established regarding the treatment of SH subjects [124, 125]. This is due to the fact that there are no data from large trials on whether and to what degree does SH affect lipid profile. Moreover, data are lacking on the overall effect of substitution therapy on morbidity and mortality in SH patients. A significant query is whether all SH patients would benefit from thyroxine replacement therapy or such therapy should be reserved for selected subgroups. Furthermore, there has not been enough evidence regarding the long-term effects of thyroid replacement in SH patients and therefore no clear recommendations can be made [126].
It seems that thyroid substitution, if used, would be most beneficial in patients with prominent thyroid dysfunction (TSH levels >10 mIU/L), higher initial cholesterol levels, smokers and subjects with positive TPO-Ab. Moreover, levothyroxine treatment may play an important role in other aspects of CVD risk beyond lipids. Of note, the potential adverse effects of levothyroxine therapy should also be taken into account. Thyroid substitution may decrease HDL-C concentration, undermining the beneficial effect of TC and LDL-C reduction in these patients. Furthermore, when treating people with angina pectoris or heart disease, one should be very cautious because thyroxin therapy may exacerbate angina or promote cardiac arrhythmia.
Overall, measurement of serum TSH levels should be included in the screening of patients with dyslipidemia [1, 127, 128]. Hypercholesterolemic patients with SH may be treated with thyroxin substitution therapy, since the restoration of euthyroidism can effectively improve lipid levels, relieve certain symptoms, and may also prevent progression to overt hypothyroidism [129].
4. OVERT AND SUBCLINICAL HYPERTHYROIDISM
The incidence of hyperthyroidism is lower (2.2%) [3] compared with hypothyroidism in the general population. Similarly, a decreased prevalence of hyperthyroidism is evident in hyperlipidemic patients, since only 3 out of the 248 patients in our study had thyrotoxicosis [25].
Despite the increased activity of the HMG-CoA reductase, levels of TC, LDL-C, ApoB and Lp(a) tend to decrease in patients with clinical or subclinical hyperthyroidism. This is due to increased LDL receptor gene expression resulting in enhanced LDL receptor-mediated catabolism of LDL particles [130, 131]. Moreover, no difference in LDL subfraction distribution has been observed between subclinical or overt hyperthyroid versus euthyroid subjects [42]. Furthermore, hyperthyroidism results in enhanced LDL oxidability, which is related to FT4 levels [46].
A decrease in HDL-C levels is also observed in hyperthyroidism, due to increased CETP-mediated transfer of cholesteryl esters from HDL to VLDL and increased HL-mediated catabolism of HDL2 [130, 131]. Triglyceride levels remain unchanged. On the other hand, no changes in blood pressure [108], Lp(a) [31] or hsCRP levels [31] have been described in hyperthyroid patients. However, an increase in factor X activity has been observed in subclinical hyperthyroidism patients, indicating a hypercoagulable state [77]. Therapy of clinical hyperthyroidism results in restoration of those alterations of lipid metabolism [130, 131], while the effects of treatment of subclinical hyperthyroidism subjects are not yet clear [132].
Iatrogenic hyperthyroidism has been associated with MI in subjects without coronary stenosis [133, 134]. Similarly, there have been case reports associating subclinical hyperthyroidism with MI [135], recurrent pulmonary embolism [136] and atrial fibrillation [135, 136].
Hyperthyroidism not only consists a significant cause of acquired hypobetalipoproteinemia, but it can also be the underlying cause of unexpected improvement of lipid profile in hyperlipidemic patients [137]. In the latter case, therapy of thyrotoxicosis restores the lipid parameters to the previously elevated levels [137].
5. CONCLUSION
Thyroid dysfunction can have an important effect on lipid profile [138]. Biochemical screening for thyroid dysfunction is critical in all dyslipidemic patients, as well as in all patients with unexpected improvement or worsening of their lipid profile. Underlying thyroid disorders should be recognized and treated in this setting.
There have been studies suggesting that screening for thyroid dysfunction is cost effective [139]. The American Thyroid Association recommends that adults be screened for thyroid dysfunction by measurement of the serum TSH concentration, beginning at age 35 years and every 5 years thereafter [140]. On the other hand, the U.S. Preventive Services Task Force concludes that the evidence is insufficient to recommend for or against routine screening for thyroid disease in adults [141].
There is a need for large studies designed to answer the question whether thyroid abnormalities (and especially SH) are associated with CVD and whether restoration of euthyroidism might influence morbidity and mortality.

