All published articles of this journal are available on ScienceDirect.

Long-term Outcome after Percutaneous Coronary Intervention Compared with Minimally Invasive Coronary Artery Bypass Surgery in the Elderly
Authors Info & Affiliations
Abstract
Background:
Elderly patients with unstable coronary artery disease (CAD) have better outcomes with coronary revascularization than conservative treatment. With the improvement in percutaneous coronary intervention (PCI) techniques using drug eluting-stents, this became an attractive option in elderly. Minimally invasive coronary artery bypass grafting (MICS-CABG) is a safe and effective alternative to conventional CABG. We aimed to explore the long-term outcomes after PCI vs MICS-CABG in ≥75 year-old patients with severe CAD.
Methods:
A total of 1454 elderly patients (≥75 year-old patients) underwent coronary artery revascularization between January 2005 and December 2009. Patients were selected in the study if they have one of the Class-I indications for CABG. Groups were divided according to the type of procedure, PCI or MICS-CABG, and 5 year follow-up.
Results:
Among 175 elderly patients, 109 underwent PCI and 66 had MICS-CABG. There was no significant difference observed in both groups with long-term all-cause mortality (31 PCI vs 21% MICS-CABG, p=0.151) and the overall 5 year survival was similar on Kaplan-Meier curve (Log rank p=0.318). The average length of stay in hospital was significantly shorter in the PCI than in the MICS-CABG group (4.3 vs 7.8 days, p<0.001). Only 4.7% of the PCI group were discharged to rehabilitation facility compared with 43.9% of the MICS-CABG group (p<0.001). The rate of repeat revascularization was significantly higher in the PCI group than in the MICS-CABG group (15 vs 3%, p=0.014).
Conclusion:
Among elderly patients, long-term all-cause mortality is similar after PCI and MICS-CABG. However, there is a significantly higher rate of repeat revascularization after PCI.
INTRODUCTION
The elderly have a higher prevalence of coronary artery disease (CAD) [1], this group of patients is progressively increasing. Despite the advantage of coronary artery revascularization in elderly patients [2-4], they have been steered towards percutaneous coronary intervention (PCI) as it is less invasive than coronary artery bypass graft (CABG) [5].
Minimally invasive coronary artery bypass (MICS-CABG) became an attractive technique for coronary revascularization. Studies have showed MICS–CABG is as effective as traditional sternotomy-based CABG [6-9]. It has the advantage of being less invasive with faster recovery and shorter hospital stays [10, 11].
We explored the long-term outcome of PCI vs MICS-CABG in an elderly population.
MATERIALS AND METHODOLOGY
From January 2005 to December 2009, 1454 elderly patients (age ≥75 years) were identified as having coronary artery revascularization for CAD at Staten Island University Hospital (Staten Island, New York). Our study only included patients with class I indications for CABG (i.e. patients with 3 vessels CAD, left main disease or 2 vessels disease with significant proximal left anterior descending lesion). In addition, patients had coronary revascularization by PCI or MICS-CABG. Those who underwent sternotomy-CABG, concomitant valve replacement/repair and prior history of PCI or CABG were excluded from the study. We followed all included patients until June 2013. The primary outcomes were all-cause mortality and rate of repeat revascularization.
After institutional review board approval, trained physicians using our hospital medical record retrieved demographic data, risk factors for CAD, co-morbidities, laboratory values, left ventricular ejection fraction, Canadian Cardiovascular Society (CCS) class and procedural information on each index case. Survival status was retrieved from our medical record and social security death index.
Statistics Analysis
Patients were divided into 2 groups according to the type of procedure and the baseline characteristics of the 2 groups were compared using the chi-square test for categorical variables and independent sample t-test for continuous variables. The distributions of continuous and categorical variables were represented as mean ± standard deviation, and frequencies and percentages, respectively.
A multivariate Cox regression was performed to explain the association between mortality and several independent variables, which have a significant association with mortality or have a clinical importance. Survival analysis was conducted using Kaplan–Meier curves and the 2 groups were compared with the use of the log rank test. All statistical analyses were performed with the use of STATA version 13.0, College Station, Texas.
RESULTS
There were 175 elderly patients, age ≥75 years, that underwent PCI or MICS-CABG who were included in the study. Among the entire cohort, 109 patients (62%) with mean age 80.6 ± 3.8 years underwent PCI and 66 patients (38%) underwent MICS-CABG with mean age 79.6 ± 3.8 years. In the PCI group, 84 patients received drug eluting stents (77%), 24 patients received bare metal stents (22%) and one patient received both types of stents. The mean number of stents used per patient was 1.5 ± 0.8. In MICS-CABG group, 54 patients (82%) underwent off-pump surgery; all patients underwent revascularization using left internal mammary artery (LIMA) as an arterial conduit and average number of grafts per patient was 2.5 ± 0.7.
Baseline characteristics are summarized in Table 1. Patients who underwent MICS-CABG had a significantly higher history of dyslipidaemia (PCI-40% vs MICS-CABG-77%, P = 0.001) while patients with PCI had a significantly higher history of myocardial infarction (PCI-46% vs MICS-CABG-24%, P = 0.004) and higher usage of clopidogrel (PCI-93% vs MICS-CABG-74%, P = 0.001). The median follow-up was 4.9 years for all patients, 34 patients (31%) died in the PCI group and 14 patients (21%) died in the MICS-CABG group (P = 0.15). Fig. (1) summarized the overall mortality outcomes in both groups.
| Variables | PCI | MICS-CABG | P Value | ||
|---|---|---|---|---|---|
| n=109 | n=66 | ||||
| Age (years) | 80.6 ± 3.8 | 79.6 ± 3.8 | 0.946 | ||
| Male | 59 | 54% | 41 | 62% | 0.3 |
| Body mass index (kg/m²) | 28.3 ± 4.9 | 26.8 ± 4.8 | 0.976 | ||
| Family history of CAD1 | 20 | 19% | 18 | 27% | 0.175 |
| Smoker | 37 | 34% | 17 | 26% | 0.256 |
| Hypertension | 86 | 79% | 59 | 89% | 0.074 |
| Diabetes mellitus | 36 | 33% | 13 | 20% | 0.057 |
| Dyslipidaemia | 44 | 40% | 51 | 77% | 0.001 |
| Peripheral arterial disease | 10 | 9% | 8 | 12% | 0.615 |
| Renal failure on dialysis | 3 | 3% | 2 | 3% | 0.915 |
| Myocardial infarction | 50 | 46% | 16 | 24% | 0.004 |
| Congestive heart failure | 11 | 10% | 4 | 6% | 0.356 |
| History of cerebrovascular event | 5 | 5% | 6 | 9% | 0.234 |
| COPD2 | 9 | 8% | 10 | 15% | 0.155 |
| Pre CCS3 | 3.0 ± 0.9 | 2.4 ± 0.9 | 0.001 | ||
| Class I | 0 | 0% | 11 | 17% | |
| Class II | 35 | 32% | 31 | 47% | |
| Class III | 39 | 36% | 14 | 21% | |
| Class IV | 34 | 31% | 10 | 15% | |
| Syntax score | 20.2 ± 7.3 | 22.9 ± 10.1 | 0.975 | ||
| Ejection fraction (%) | 46.7 ± 12.6 | 42.9 ± 11.4 | 0.976 | ||
| Preoperative creatinine (mg/dl) | 1.3 ± 0.9 | 1.1 ± 0.4 | 0.944 | ||
| Preoperative glucose (mg/dl) | 146 ± 47 | 107 ± 38 | 1 | ||
| Aspirin | 103 | 97% | 64 | 97% | 0.899 |
| Clopidogrel | 99 | 93% | 49 | 74% | 0.001 |
| Beta blocker | 81 | 76% | 58 | 88% | 0.066 |
| ACEI4 or ARBS5 | 88 | 83% | 60 | 91% | 0.157 |
| Statin | 85 | 80% | 63 | 95% | 0.007 |
| Site of lesion | 0.001 | ||||
| Left main artery | 2 | 2% | 3 | 5% | |
| Two vessels, including proximal LAD | 54 | 50% | 12 | 18% | |
| Three vessels | 53 | 49% | 51 | 77% | |
| Number of bypass grafts | |||||
| 1 | 5 | 8% | |||
| 2 | 30 | 45% | |||
| 3 | 27 | 41% | |||
| 4 | 4 | 6% | |||
| Type of stent | |||||
| BMS6 | 24 | 22% | |||
| DES7 | 84 | 77% | |||
| Both | 1 | 1% | |||
| Internal mammary artery utilized | 66 | 100% | |||
| Cardiopulmonary bypass | 12 | 18% | |||
1 CAD denotes coronary artery disease
2 COPD denotes chronic obstructive pulmonary disease
3 CCS denotes Canadian Cardiovascular Society
4 ACEI denotes angiotensin converting enzyme inhibitor
5 ARBS denotes angiotensin II receptor blockers
6 BMS denotes bare metal stent
7 DES denotes drug eluting stent
The average length of stay in the hospital was significantly shorter in the PCI group, 4.3 ± 4.7 days, than in MICS-CABG group, 7.8 ± 7.4 days, (P < 0.001). In addition, 5 patients (4.7%) in the PCI group were discharged to a rehabilitation facility compared with 29 patients (43.9%) in the MICS-CABG group (P < 0.001).
During the entire follow-up, 16 patients (15%) in the PCI group needed repeat revascularization, compared with 2 patients (3%) in MICS-CABG group, (P = 0.014). The Kaplan-Meier curve showed no significant difference in overall survival between both groups (log rank P = 0.318) (Fig. 2).
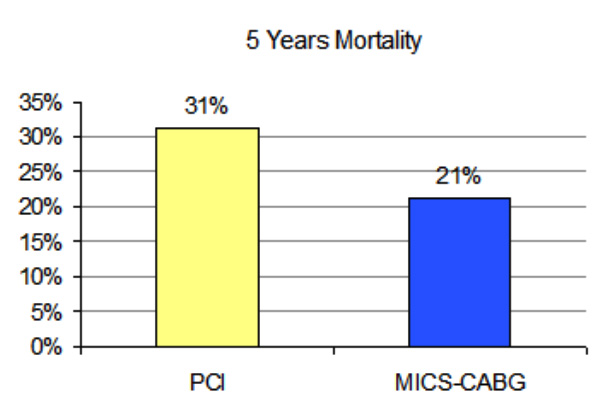
Long term mortal ity in elderly patients underwent PCI and MICS-CABG (P=0.150).
By using a multivariate Cox-regression model for all-cause mortality among elderly patients, including all possible predictors of mortality, age and ejection fraction were the only predictors of mortality in our study population, but the type of the procedure was not predictive of mortality with a hazard ratio of 0.77 (CI 0.28-2.10) (Table 2).
DISCUSSION
In our study, we compared 2 different procedures for coronary revascularization, PCI and MICS-CABG, in elderly patients with an average age of 81 years. We found that patients that underwent PCI had similar long-term outcome as MICS-CABG, there was no significant difference between both groups regarding all-cause mortality (31% PCI vs. 21% MICS-CABG; P = 0.15) and the overall 5 year survival was similar on Kaplan-Meier curves. Patients who underwent PCI had shorter hospital stay and less discharge to rehabilitation facility but had a higher rate of repeat revascularization.
Many trials, including the SYNTAX (The synergy between percutaneous coronary intervention with Taxus and cardiac surgery) trial, comparing CABG with PCI showed all-cause mortality benefit and cardiac-related mortality benefit after CABG compared with PCI [12-16]. Similarly, the ASCERT (The American College of Cardiology Foundation and the Society of Thoracic Surgeons Database Collaboration on the Comparative Effectiveness of Revascularization Strategies) study was an observation study which showed that among elderly patients (age ≥65 years) with multivessel disease had lower mortality and a long term survival benefit after open thoracotomy CABG compared with PCI [17]. In addition, in a meta-analysis of 10 randomized trials Hlatky et al. demonstrated long term mortality benefit after CABG compared with PCI in elderly patients ≥65 years [18]. But, Alam [19], explored the outcome between PCI and CABG in elderly >70 years after revascularization for unprotected left main coronary artery disease, and found no significant difference between both procedures regarding all-cause mortality.
Studies showed the rate of repeat revascularization is higher after PCI compared with CABG, in a meta-analysis of 9 observational studies, Benedetto [20] found the frequency of repeat revascularization was more than 3 times higher after PCI than CABG. Similarly, Bravata [21], in a systematic review of 22 randomized controlled trials found similar results after 5 years of follow up. Fosbøl [22] studied the rate of repeat revascularization in older adults with an average age of 73 years and found that advanced age has a lower rate of repeat revascularization after CABG. In addition, Harskamp [23] in a meta-analysis comparing minimally invasive CABG with PCI which in LAD disease only, found a higher rate of repeat revascularization after PCI. An angiographic patency study with consecutive patient undergoing MICS-CABG, showed patency of 100% for LIMA and 92% for all grafts, with 6 month computed tomography angiographic follow-up, conferring longevity to the CABG procedure and symptom free survival [10].
| Hazard Ratio | 95% Confidence Interval | P Value | ||
|---|---|---|---|---|
| PCI1 vs. MICS-CABG2 | 0.77 | 0.28 | 2.10 | 0.616 |
| Age | 1.14 | 1.05 | 1.25 | 0.002 |
| Gender (Male) | 1.02 | 0.49 | 2.15 | 0.949 |
| Dyslipidaemia | 0.60 | 0.27 | 1.36 | 0.226 |
| Smoking | 1.26 | 0.61 | 2.60 | 0.527 |
| Diabetes mellitus | 1.84 | 0.88 | 3.83 | 0.106 |
| Hypertension | 1.81 | 0.87 | 3.81 | 0.115 |
| Myocardial infarction | 2.00 | 0.97 | 4.10 | 0.060 |
| Congestive heart failure | 0.40 | 0.12 | 1.30 | 0.128 |
| Ejection fraction | 0.97 | 0.94 | 1.00 | 0.028 |
| Preop CCS3 | 0.73 | 0.46 | 1.16 | 0.186 |
| Site of the lesion | 1.81 | 0.87 | 3.81 | 0.115 |
| Aspirin | 1.05 | 0.21 | 5.23 | 0.955 |
| Clopidogrel | 2.96 | 0.63 | 13.86 | 0.167 |
| Beta blocker | 2.02 | 0.23 | 17.61 | 0.525 |
| ACEI4 or ARBS5 | 0.29 | 0.03 | 2.67 | 0.277 |
| Statin | 2.56 | 0.79 | 8.30 | 0.116 |
1 PCI denotes percutaneous coronary artery intervention
2 MICS CABG denotes minimal invasive cardiac surgery - coronary artery bypass graft
3 CCS denotes Canadian Cardiovascular Society
4 ACEI denotes angiotensin converting enzyme inhibitor
5 ARBS denotes angiotensin II receptor blockers
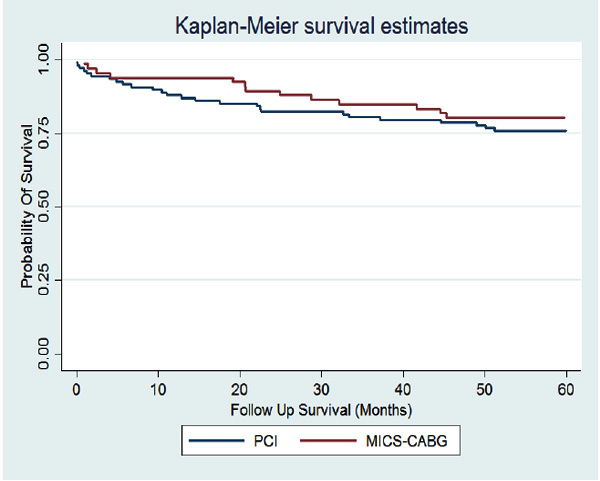
Kaplan-Meier curve of survival in elderly patients underwent PCI and MICS-CABG (P = 0.318).
Elderly patients with CAD usually have co-morbid conditions and after sternotomy CABG they have a high incidence of complications and longer hospital stay than younger patients [24-27]. King [28] found the length of hospital stay after minimal invasive CABG and PCI is shorter than for sternotomy CABG; and Alam [19] found that elderly patients aged >70 years had an average hospital stay of 4.2 days, but longer hospital stay after sternotomy CABG (8.3 days).
Quality of life is an important factor for the elderly. Bardakci [29], showed that octogenarians undergoing CABG are less likely to be discharged home compared with younger patients. Gopaldas [30], showed that 45% of elderly patients aged ≥80 years were transferred to rehabilitation or care facility after CABG. Although early recovery after MICS-CABG is a documented advantage over traditional CABG, not enough studies in the elderly have elucidated this.
Our study has several limitations. First, because of the small number of patients, we could not carry out a subgroup analysis to explore the effect of procedure in patients with left main disease or 3 vessels disease alone. However, we repeated the statistical analysis after adding patients with previous history of PCI and the results were similar. Secondly, this study is non-randomized and retrospective in nature, we cannot exclude the possibility of selection bias. Third, we explored all-cause mortality without considering cardiac causes of death. Using the social security death index and medical records to detect the mortality, could lead to missing some outcomes.
Among elderly patients who underwent coronary revascularization, there was no significant difference regarding long term all cause mortality or survival after MICS-CABG and PCI. However, patients who underwent PCI had shorter hospital stay and fewer discharges to rehabilitation facilities but they had higher rate of repeat revascularization. Further evaluation on a large scale in this group of patients is needed.
CONFLICT OF INTEREST
J.T.M. reports lecture fees from Medtronic. All other authors have nothing to disclose with regard to commercial support.
ACKNOWLEDGEMENTS
Declared none.

