All published articles of this journal are available on ScienceDirect.

High Prevalence and Diminished Awareness of Overweight and Obesity in a Mediterranean Population. An Alarming Call for Action
Authors Info & Affiliations
Abstract
Introduction:
The epidemic proportions of overweight, obesity and diabetes in most European countries stress the need for the implementation of an effective action plan for the prevention of cardiovascular (CV) disease. This ques-tionnaire study was designed to evaluate the viewpoint of the general population regarding the relative significance of CV risk factors in the cumulative risk of CV disease.
Methods:
All participants answered a questionnaire regarding the self-reported presence of CV disease risk factors and the perceived notion of having excess weight. They were also asked to list CV disease risk factors, ranking them in order of perceived relative significance. Participants were also subjected to total cholesterol measurement using a portable total cholesterol testing meter.
Results:
The survey population consisted of 32,736 individuals (49.1% males). According to participant self reporting, 32.9% were smokers, 24.7% had hypertension, 9.8% had diabetes, 74.8% reported having stress, 41.9% had insufficient physical activity and 43.3% had hyperlipidemia. The prevalence of overweight was 43.9% and the prevalence of obesity (BMI ≥30 kg/m2) was 18.6%. Only 24.4% of participants reported that they had excess weight. The 45.2% of the ques-tioned individuals considered that stress was the most important CV risk factor.
Conclusions:
Despite the high prevalence of overweight and obesity, the majority of participants were unaware of the contribution of these well-established risk factors to the occurrence of CV disease. Improving public awareness is impor-tant in order to control the epidemic proportions of these modifiable risk factors.
1. INTRODUCTION
Despite the significant decline of cardiovascular disease (CVD) mortality achieved in the last 50 years, largely reflecting advances in therapeutic management, the outcome of primary prevention efforts in the majority of the European countries has been modes [1] . In particular, the incidence of CVD has declined in some of the Northern European countries, but it has been stable or even increased in some others, especially in Eastern Europe [2]. Although the large-scale campaigns aiming to tackle the major cardiovascular (CV) risk factors have proved effective, at least in some European countries, the need for additional efforts is imperative since the prevalence of diabetes and obesity have increased dramatically among European populations largely due to nutrition changes, urbanization and socioeconomic changes [3].
A better understanding and priority ranking of the reasons promoting unfavorable diet and exercise behavior is a prerequisite for the development and implementation of an efficient action plan targeting CVD prevention. Improving awareness of the well-established association between obesity and hypertension [4], diabetes [5] and atherosclerosis [6] should be set as top priority in the agenda of CVD prevention. Patient underestimation of the significance of major CVD risk factors including obesity, diabetes, smoking and sedentary lifestyle is partly responsible for the adoption of detrimental lifestyle behavior. The evaluation of a population’s viewpoint will uncover potential education gaps, thus enabling proper redirection of health care provision. Improved public education will provide motivation to the general population to avoid weight gain.
The need for defining a population perspective in ranking the relative importance of the CV risk factors provided the rationale for the design and conduct of this descriptive questionnaire study.
2. MATERIALS AND METHODS
Data were derived from a population-based coronary risk factor screening program (descriptive questionnaire study) conducted in 6 urban areas (Athens, Korinthos, Thessalonica, Alexandroupoli, Trikala and Corfu) in Greece. Screening of participants took place in high-traffic areas such as central squares and underground stations. The data were collected by specifically trained physicians, and blood samples were taken by research nurses. All individuals answered a questionnaire regarding demographics (age, sex, weight, height) and the self-reported occurrence of CVD risk factors (smoking status, diabetes mellitus, dyslipidemia, hypertension, family history of premature coronary artery disease, sedentary lifestyle). Survey participants were also asked to list CVD risk factors, ranking them in order of perceived relative significance. In order to assess their perceived notion of having excess weight they were asked the following question “Do you believe you have excess weight?” Participants were also subjected to total cholesterol measurement using a portable total cholesterol meter (Accutrend plus System®, Roche Diagnostics) using a drop of blood from a finger prick. The range of measurable cholesterol levels was from 150 to 300 mg/dl.
Participants were defined as overweight or obese according to their body mass index (BMI). Individuals with a BMI < 25 kg/m2 were classified as being of normal weight, those with a BMI ≥ 25 and <30 kg/m2 were categorized as overweight and those with a BMI ≥ 30 kg/m2 were defined as obese.
All participants gave their informed consent and signed an agreement form for the blood samples that were collected for the measurement of cholesterol levels. The study was conducted under the auspices of the Hellenic Heart Foundation.
Statistical Analysis:
Values are expressed as means ± SD unless otherwise specified. Using the independent Samples t-test, we compared parameters between overweight and normoweight. Spearman’s correlation coefficient was used to evaluate the bivariate relationships. A two-sided p <0.05 was considered as significant. Data analysis was performed using SPSS 15.0 software (SPSS Inc., Chicago, IL).
3. RESULTS
I. Baseline and Self-reported Characteristics
The study population included 32,736 individuals (49.1% males). The baseline characteristics of the survey participants are presented in Table 1. In the total population, only 37.3% had a normal weight (BMI <25), while the prevalence of overweight was 43.9% (48.5% ♂/ 35.4 ♀), and the prevalence of obesity was 18.6% (20.0% ♂/ 17.2 ♀).
Baseline Characteristics of the Survey Participants
| Whole Population | Males | Females | |
|---|---|---|---|
| Age (years) | 53.1±14.8 | 55±14 | 53±13 |
| Weight (kg) | 75.5±14.3 | 83.1±12.6 | 68.7±12.2 |
| Height (cm) | 168±9 | 174±7 | 162±6 |
| BMI (kg/m2) | 26.7±4.2 | 27.4±3.6 | 26.1±4.5 |
| Cholesterol (mg/dl) | 199.5±33.9 | 195.1±32 | 203.4±34 |
Values are expressed as means ± SD
Ranking of Cardiovascular Risk Factors in Different Subgroups of Paricipants
| Stress | Smoking | Hypertension | Diabetes | Hyperlipidemia | Sedentary Lifestyle | Obesity | |
|---|---|---|---|---|---|---|---|
| Males | 29.7 % | 17 % | 6.5 % | 4.4% | 14.3 % | 5.0 % | 7.6 % |
| Females | 35.9 % | 14.6 % | 5.4 % | 2.4 % | 16.6 % | 4.0 % | 8.4 % |
| Age<50 years | 36.1 % | 20.4 % | 2.6 % | 1.5 % | 9.8 % | 5.3 % | 8.3 % |
| Age≥50 years | 30.7 % | 12.5 % | 8.4 % | 4.7 % | 19.6 % | 3.8 % | 7.8 % |
| Smokers | 29.1 % | 39.0 % | 3.3 % | 2.4 % | 10.0 % | 3.0 % | 5.9 % |
| Non smokers | 34.9 % | 3.9 % | 7.2 % | 3.9 % | 18.5 % | 4.8 % | 9.3 % |
| Hypertensive | 26.6 % | 10.9 % | 21.6 % | 5.5 % | 17.7 % | 2.6 % | 8.4 % |
| Overweight | 27.1 % | 11.9 % | 7.6 % | 4.3 % | 14.5 % | 4.2 % | 21.9 % |
| Diabetics | 21 % | 12.3 % | 7.5 % | 26.9 % | 16.7 % | 2.6 % | 7.7 % |
| Hyperlipidemic | 31.8 % | 15.6 % | 5.6 % | 3.0 % | 19.3 % | 4.1 % | 8.3 % |
According to self reporting, 34.2 % were smokers (34.9% ♂/33.5 ♀), 25.6% had a family history of premature coronary artery disease (22.1% ♂/28.6% ♀), 25.2% had hypertension (26.7% ♂/23.6 ♀), 9.9% had diabetes (12% ♂/7.8% ♀), 76.4% reported having stress (69.7% ♂/82.7 ♀), 42.2% (40.7% ♂/43.6 ♀), had insufficient physical activity and 45.9 had hyperlipidemia (43.3% ♂/48.2 ♀) (Fig. 1).
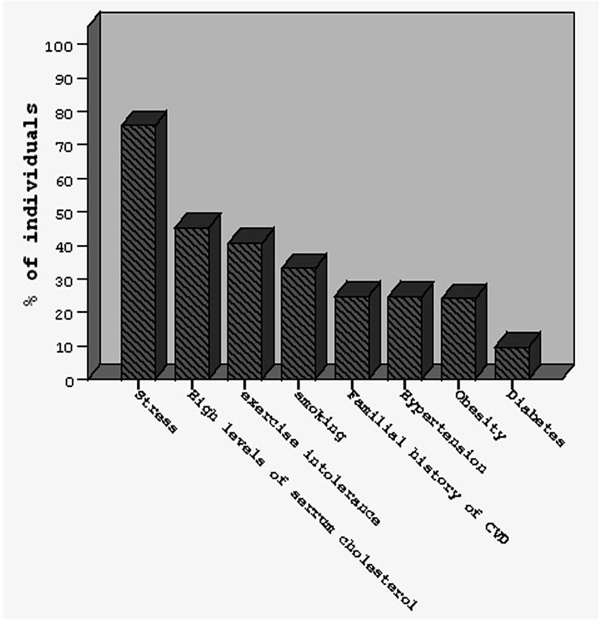
Prevalence of the major cardiovascular risk factors in the cohort of the study.
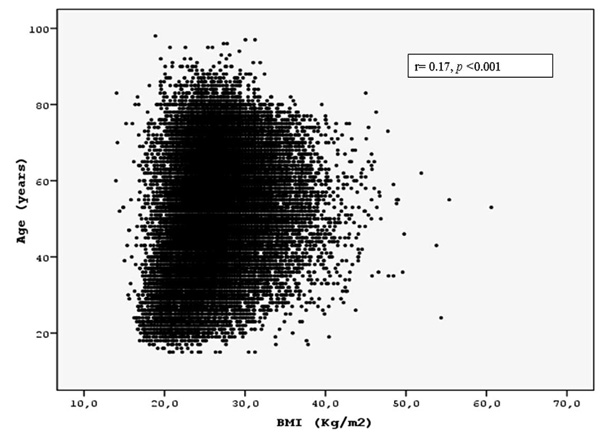
Scatter graph of BMI in kg/m2 versus age.
The majority of overweight and obese people also had a combination of other risk factors. Specifically, 4.3% also had hyperlipidemia, hypertension and were smokers, 6.5% had diabetes and hyperlipidemia, 6.0% had hypertension and diabetes, 13.5% had hyperlipidemia and were smokers, 13.08% had hypertension and sedentary lifestyle, 14.5% were smokers and had sedentary lifestyle , 20.4 % had hyperlipidemia and sedentary lifestyle and 16.5% had hypertension and hyperlipidemia. Finally, a total amount of 213 from the 18348 obese and overweight individuals (1.1%) also had the other 5 risk factors (smoking, diabetes, hyperlipidemia, sedentary lifestyle and hypertension)
Only 24.4% of individuals answered positively to the question whether they believed that they had excess weight. The percentage of overweight and obese participants who answered positively to the same question was 71.8%. Furthermore, only 58.1% of participants who had cholesterol level ≥190 mg/dl answered positively to the question whether they had hyperlipidemia.
II. Ranking of Cardiovascular Risk Factors in Order of Relative Significance
The answers to the question “Which is the more significant risk factor for CVD?” show that 32.9% believed that stress was the most dangerous, 15.7% smoking, 15.5% hyperlipidemia, 8.0% excess weight, 5.9% hypertension, 4.7% a family history of premature coronary artery disease, 4.4% sedentary lifestyle and 3.4% diabetes. Table 2 shows the ranking of CV risk factors in different subgroups of individuals
III. Overweight and Comorbidities
A significantly higher percentage of self-reported hypertensives had a BMI ≥ 25 kg/m2 compared with those with a normal weight (77.0 vs 42.4%, p < 0.001). The mean BMI of hypertensives was 28.1 ± 4.1 vs 26.1 ± 4.1 kg/m2 (p < 0.001) in non hypertensives. Furthermore, a significantly higher percentage of self-reported diabetics were overweight or obese compared with those with a normal BMI (75.3 vs 43.6%, p < 0.001). The mean BMI of diabetic patients was 28.2 ± 4.4 vs 26.4 ± 4.1 kg/m2 (p < 0.001) in non-diabetic subjects.
In younger individuals (age <30 years old) the mean BMI was significantly lower than for the elderly (25.7 ± 4.4 vs 27.2 ± 4.1 kg/m2, p<0.001). However, there was no significant difference in BMI between smokers and non-smokers (26.1 ± 4.2 vs 26.8 ± 4.2 kg/m2, p = 0.09).
Spearman’s correlation coefficient comparisons revealed statistically significant correlation of BMI with age, (r = 0.17, p < 0.001, Fig. 2) and with diabetes (r = 0.11, p < 0.001) and hypertension (r = 0.22, p < 0.001).
4. DISCUSSION
Our primary finding is the high prevalence of overweight and obesity in the survey population associated with a impaired awareness of the relative contribution of obesity, and overweight in the cumulative risk of CVD.
Obesity – Overweight
Obesity is a worldwide epidemic. According to a recent press release issued by the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics, 2 in 5 Americans at the 55 to 64 age group are obese [7]. Similar are the findings of our study (21.8% of the obese people were between 55 and 64 years old and 22.6 % of people between 55 and 64 years old were obese).
A worse scenario is anticipated in the near future since the long term (30-year) risk for developing overweight or obesity in adults with a normal BMI exceeded 50 and 25%, respectively in the Framingham Heart Study [8]. However, apart from the BMI, emphasis should be given to the selective accumulation of fat in the abdominal region which is included in the cluster of traits defining metabolic syndrome (MetS)[9]. Based on the results of the INTERHEART study, the presence of abdominal obesity doubles the risk of a heart attack and is considered as a more significant risk factor for heart attack compared with the BMI [10]. According to the NCEP ATPIII definition, abdominal obesity, as estimated by waist circumference, is one of the MetS characteristics [11] . The MetS is associated with increased risk of atherosclerotic CVD and type 2 diabetes mellitus [11,12]. It is of crucial importance that weight loss can improve all features of the MetS and consequently exert a beneficial effect on its associated comorbidity [13]. Disseminating information on the detrimental effects of weight gain, as well as abdominal obesity and MetS, is necessary in order to retain a minimum level of vigilance in the general population which will partly enhance primary and secondary prevention of obesity and overweight.
According to the findings of the MetS-Greece Multicenter study, the MetS is highly prevalent among Greek adults, with an estimated age-standardized prevalence of 23.6%, while abdominal obesity was met in 82% of cases, rendering it the most common trait of MetS [14]. In a survey conducted among Greek medical students, approximately 40% of men and 23% of women were overweight, while central obesity was found in 33.4% of male and 21.7% of female students [15]. Furthermore, the ATTICA survey, having included a representative and random sample of 3,042 Greek adults from the ATTICA region, concluded that the prevalence of overweight and obesity were 53 and 20% in men and 31 and 15% in women [16]. These results are confirmed from our study. The prevalence of overweight and obesity in our study were 48.5 and 20% in men and 35.4 and 17.2% in women.
Special emphasis should also be addressed to childhood obesity since today’s prevalence of childhood obesity may represent tomorrow’s prevalence of diabetes and coronary artery disease. Epidemiologic data are disappointing since more than 550,000 children are affected by MetS [17], 3 million school-age children in the European Union (EU) are obese, [18] and the number of overweight children in the EU is rising by around 400,000 per year [19]. In Greece, the prevalence of overweight and obesity has been estimated to be 35.6 and 6.7% among boys and 25.7 and 6.7% among girls, respectively [20], while these rates have exhibited a rising trend by 63 and 202%, respectively in the last 20 years as calculated in a randomly selected sample from Crete [21]. The lack of exercise is also another characteristic of Western type way of life and plays a main role in the pathogenesis of obesity and CVD. In our sample, 42% reported no or little physical activity.
In our population, the prevalence of obesity was 18.6% while the combined prevalence of overweight and obesity was 62.7%. Among US adults the respective rates estimated in 1999-2002 were 30.4 and 65.1%, respectively [22], denoting that obesity represents a worldwide public health issue, primarily determined by the Western-type way of living, the latter having attenuated potential fluctuations and disparities in prevalence attributed to racial, ethnic, genetic and environmental characteristics. Taking also into consideration that self reported surveys tend to significantly underestimate the prevalence of overweight and obesity due to inherent limitations related to reporting and systematic bias [23], the scale of the problem in our country might even be worse.
The majority of the questioned individuals considered that stress was the most important CV risk factor, underestimating the role of obesity, diabetes mellitus and smoking and they were also unaware of the unfavorable effect of sedentary lifestyle and poor exercise in CV risk profile. In contradiction to our results an American Heart Association (AHA) national telephone survey among women demonstrated that overweight status and lack of exercise were most often identified as risk factors for heart disease by 41 and 40% of participants, respectively, while stress was cited as a major risk factor only by 18% of women [24].
An interesting finding in our study was that only the individuals who have a risk factor (smokers, diabetics and hypertensives) were more aware of risk factors and have better risk factor stratification although even in those stress is very popular answer as the most dangerous risk factor. These 3 subgroups of participants are the only subgroups where stress is not placed at the top of the list of risk factor grading. It is worth noting that in our study, although 63% of participants were overweight, only a quarter of them considered that they had excess weight, a finding which was also documented in the subgroup of obese subjects. Moreover, only the half of the individuals who have high cholesterol level according to our measurement considered that they had hyperlipidemia. The documented paradox between the actual and perceived weight status validates the limited awareness of optimal weight in the broad population. These findings could partly explain the adoption of unfavorable health behaviors in our country which, combined with a change in dietary habits away from the traditional Mediterranean diet, have contributed to the substantially increasing burden of obesity [25].
Clinical Implications
The impaired perception of the relative significance of coronary risk factors in combination with the overestimation of the role of stress emphasize the need for the development and implementation of a CVD preventive strategy aiming to increase awareness and promote favorable lifestyle modifications. Following the American Heart Association (AHA)/ National Heart Lung and Blood Institute (NHLBI) recommendations, the mitigation of modifiable metabolic vascular risk factors (obesity, physical inactivity, and atherogenic diet) should be set among primary goals of clinical management [26-28]. The key point is that improved knowledge is expected to translate into active lifestyle modification among affected individuals, thus tackling the worsening epidemic of obesity and its associated comorbidities. The primary significance of obesity and diabetes prevention should be addressed in governmental policies, educational programs and social services provided to the broad population.
Among the plethora of environmental factors which contribute to the formation of nutritional attitude, especially among children, advertising plays a major but potentially reversible detrimental role. Unfortunately, children are considered by the food industry as a highly exploitable market group [29]. International task forces should develop advertising guidelines with the intention to restrain food and beverage marketing which drives most children and adolescents away from achieving basic nutritional goals. However, governments should take advantage of the effect that mass media exert on children’s preferences and nutritional profile, by promoting legislations which mandate the promotion of healthy diets. A nationwide public health campaign should be initiated with a special emphasis on television, magazines and newspapers since mass media have been reported as the most commonly cited source of information about heart disease and stroke [10,24].
The major study limitation is that the participants were not randomly selected and thus are not representative of the general population. Despite the risk of selection bias, the actual ratio of prevalence to awareness might be even higher among the general population, since the survey took place in urban areas without representatives from rural areas where awareness regarding health issues is likely to be lower [30].
In conclusion, this survey demonstrated a high prevalence of overweight and obesity and diminished awareness that overweight and obesity promote the occurrence of CVD. CV mortality in Europe in the next decades is expected to be heavily influenced by the increasing prevalence of overweight and obesity. Tackling this epidemic through a multilateral approach, including the amelioration of public awareness on the significance of these CV risk factors, should pave the way to prevention of CVD.
CONFLICT OF INTEREST
During the last 6 years GA has received honoraria from Pfizer Hellas SA for participating in satellite symposia and advisor boards.
AKNOWLEDGEMENTS
None Declared.

