All published articles of this journal are available on ScienceDirect.

Rigid Sternal Fixation Improves Postoperative Recovery
Authors Info & Affiliations
Abstract
Introduction:
During the past five years, ridged sternal fixation has been utilized for sternal closure after cardiac surgery. It is known that this procedure provides better sternal stability; however, its contribution to patient recovery has not been investigated.
Methods:
Retrospective chart review was conducted for patients who underwent CABG and/or valve surgery in our institution between 2009 and 2010. Preoperative, perioperative, and follow-up data of patients with ridgid fixation (group R, n=89) were collected and compared with those patients with conventional sternal closure (group C, n=133). The decision regarding the sternal closure method was based on the surgeon’s preferences. Univariate followed by multivariate analyses were performed to evaluate the dominant factor of sternal lock usage and to evaluate postoperative recoveries. The factors included in the analyses were; age, sex, coronary risk factors, urgency of surgery, ejection fraction, coronary anatomy, preoperative stroke, renal function, and preoperative presence of heart failure. All statistical analyses were performed by JMP software.
Results:
Group R was younger (62 ± 9 in group R vs 69 ± 11 in group C, p<0.0001) than group C, more male dominant (61% vs 49%, p=0.0452), had a lower percentage of patients undergoing redo-surgery (2.2% vs 9.0%, p<0.0418), was more likely to be used in isolated coronary artery bypass grafting (71% vs 46%, p=0.0002), more often to be used for large patient (body mass index, BMI greater than 30) (58% vs 37%. P=0.0045), and patients were more likely to have a low EuroSCORE (2.6 ± 2.3 vs 4.4 ± 2.7). Intubation time (13 ± 20 hours vs 39 ± 97 hours, p=0.0030), ICU stay (58 ± 40 hours vs 99 ± 119 hours, p=0.0003), and postoperative length of stay (7.0 ± 3.7 days vs 8.4 ± 4.7 days, p<0.0141) were significantly shorter in group R than group C. Multivariate analyses showed ridged sternal fixation was the most dominant factor affecting intubation time and ICU stay.
Conclusion:
Rigid sternal fixation systems were more frequently applied to low risk young male patients. Among these selected patients, ridgid sternal fixation can contribute to early patient recovery.
INTRODUCTION
Conventionally, the sternum has been closed with stainless steel wires after open heart surgery. In most patients, the stainless steel wire closure is sufficient to provide sternal reapproximation and stability. However, the wire can fracture or may cut through the sternum by excessive coughing or pulmonary toileting, which causes sternal dehiscence, although it is rare. Even if the wire and bone remain intact, the wires may become loose because of the wire cutting into the cortex of the sternum or because of a rolling motion of the sternum due to the respiratory motion of the thorax [1]. Incomplete sternum cooptation may lead to sternal instability, sternal pain, delay in the recovery of the patient’s daily activity, and increased risk of sternal dehiscence and infection. [2, 3]. This sternal instability may occur right after chest closure or weeks after surgery depending on the quality of the sternum, presence of osteoporosis in the sternum, and closure technique. Numerous techniques have been introduced to reduce mechanical stress to the sternum caused by sternal wire circulage [2-6].
Recently, a rigid fixation method using sternal plates was introduced. Rigid fixation requires metal plate and screws to stabilize the sternum. The plate functions as an additional skeletal brace over the sternum to hold the hemisternum together. Compared to the wire closure which is linear and provides a single point of support, rigid fixation provides two-dimensional support using a metal plate. Cadaver study showed that the rigid plate fixation provided better stability of the sternum after median sternotomy than wire circulage [7]. Once the plate is placed on the sternum by screws, the titanium plate will not break. Previous clinical study demonstrated a lower incidence of sternal infection in the group undergoing sternal plating compared that in those receiving conventional sternal wiring [8, 9].
Rigid fixation was introduced at our institution in 2006 and recently has been used more frequently. In this study, we investigated the types of patients more likely to be closed by rigid fixation and analyzed their outcomes in comparison to those whose sternum was closed using wires.
METHODS
Rigid Sternal Closure
The Sternalock (Biomet Microfixation, Jacksonville, FL), approved for sternal closure by the US Food and Drug Administration, has been used for the rigid sternal closure in our institution. Detains of sternal closure technique using the Sternalock has been published elsewhere [10]. Briefly, the quality of the sternum was evaluated by a surgeon to make sure the bone marrow of the sternum has sufficient density to hold the screw. The peristernal fascia was elevated from the anterior table of the sternum using electrocautery. The thickness of the sternum was measured and a thickness between 4mm and 14mm was eligible to rigid closure. Two stainless steel wires were placed in the upper manubrium and at least one stainless steel wire was placed in the lower body of the sternum to reapproximate the sternum. After reapproximation of the sternum by twisting wires, the lateral sternum edges at the 4th or 5th intercostal space was grasped with a sternal re-approximation grasper to maintain the sternal alignment. At least 1 plate was placed at the manubrium and at least 2 plates on the body of the sternum. The configuration of the plates was individualized based on the size and shape of the sternum. The plates were bent to seat onto the surface of the sternum and secured to the sternum with self-tapping screws. The appropriate length for the screws was sternum thickness plus 4 mm, so that the screw could penetrate both the anterior and posterior cortex of the sternum. The screws were placed using a battery driven automatic driver. The decision regarding the sternal closure method was based on the surgeon’s preferences.
Wire Sternal Closure
Conventional sternal closure was performed using 6-8 stainless steel wires (Ethicon, San Antonio, TX). Usually, 2-3 wires were paced on the manubrium, and 5-6 wires were placed into the intercostal space of the body of the sternum, using a single circulage technique.
Patients
Retrospective chart review was conducted for patients who underwent coronary artery bypass grafting (CABG) and/or valve surgery between 2009 and 2010 in our institution. Preoperative, perioperative, and follow-up data of patients were collected from a database that was approved for use in research by the internal review board. Patients who underwent ridgid fixation (group R) were compared with those of who underwent wire closure (group C).
Statistical Analyses
The factors included the analyses were; age, sex, body mass index, coronary risk factors (hypertension, diabetes, insulin use, smoking history), urgency of surgery, ejection fraction, coronary anatomy, valvular pathology, other comorbidities (preoperative stroke, renal function, and preoperative presence of heart failure), and surgery method (CABG, number of distal anastomoses, aortic valve surgery, and mitral valve surgery). Univariate followed by multivariate analyses were performed to identify the dominant factors influencing the selection of rigid fixation and to analyze postoperative outcomes. P value less than 0.05 was considered significant. Risk factors with a p-value less than 0.05 on univariate analyses were further analyzed by multivariate analyses to identify independent risk factors. Factors closely linked to other factors such as EuroSCORE were excluded from the multivariate analyses. All statistical analyses were performed using JMP software (SAS, Cary, NC).
RESULTS
A total of 222 patients underwent coronary with or without valve surgery. Among them, 89 patients underwent rigid sternal fixation (group R) and 133 patients underwent conventional closure. These demographics are showed in Table 1. The characteristics of the two groups were different. Univariate analyses showed that patients in group R were younger (62 ± 9 in group R vs 69 ± 11 in group C, p<0.0001), more male dominant (61% vs 49%, p=0.0452), undergone redo-surgery less frequently (2.2% vs 9.0%, p<0.0418). Furthermore, rigid fixation was more often performed in a large patient (body mass index, BMI greater than 30) (58% vs 37%. P=0.0045), more likely performed after coronary artery bypass grafting (71% vs 46%, p=0.0002), less likely to be performed after valve surgery (12% vs 32%, p=0.0002), and more likely to be performed patients with low EuroSCORE (2.6 ± 2.3 vs 4.4 ± 2.7) than group C. Further multivariate analyses showed age less than 65, male sex, and BMI greater than 30 were independent factors favoring the use of ridgid sternal fixation.
Patients Demographics
| Rigid Fixation | Conventional Closure | Univariate | Multivariate | |
|---|---|---|---|---|
| Group R | Group C | Analyses | Analyses | |
| Number of patients | 89 | 133 | P value | P value |
| Clinical characteristics | ||||
| Age (mean ± std) | 62 ± 9 | 69 ± 11 | <0.0001 | |
| Age over 75 | 8 (9%) | 47 (35%) | <0.0001 | 0.0097 |
| Age under 65 | 55 (62%) | 48 (36%) | 0.0002 | 0.0002 |
| Male sex | 75 (84%) | 64 (48%) | <0.0001 | 0.0001 |
| Cardiac profile | ||||
| Acute myocardial infarction | 5 (6%) | 5 (4%) | 0.5129 | |
| History of congestive heart failure | 11 (12%) | 15 (11%) | 0.8060 | |
| Poor ejection function (<40%) | 10 (11%) | 20 (15%) | 0.4168 | |
| Atrial fibrillation | 6 (7%) | 20 (15%) | 0.0596 | |
| Redo surgery | 2 (2%) | 12 (9%) | 0.0418 | 0.0598 |
| Emergent or urgent surgery | 16 (18%) | 35 (26%) | 0.1478 | |
| Left main disease | 15 (17%) | 20 (15%) | 0.7159 | |
| Coronary risk factors | ||||
| Hypertension | 76 (85%) | 117 (88%) | 0.5766 | |
| Diabetes | 27 (30%) | 51 (38%) | 0.2206 | |
| Insulin user | 7 (8%) | 20 (15%) | 0.1091 | |
| Hyperlipidemia | 75 (84%) | 99 (74%) | 0.0811 | |
| Smoking | 18 (20%) | 18 (14%) | 0.1850 | |
| Body mass index above 30 | 50 (56%) | 49 (37%) | 0.0045 | 0.0048 |
| Body mass index above 35 | 18 (20%) | 24 (18%) | 0.6845 | |
| Family history | 50 (56%) | 63 (47%) | 0.1981 | |
| Peripheral vascular disease | 12 (14%) | 13 (10%) | 0.3916 | |
| Cerebral vascular accident | 11 (12%) | 22 (17%) | 0.3907 | |
| Chronic pulmonary disease | 15 (17%) | 27 (20%) | 0.5205 | |
| Renal dysfunction (Creatinine above 1.5 mg/dl) | 2 (2%) | 6 (5%) | 0.3751 | |
| Surgery | ||||
| Coronary artery bypass surgery | 73 (82%) | 84 (63%) | 0.0025 | 0.5381 |
| Internal mammary artery use in coronary bypass | 69 (95%) | 68 (83%) | 0.0284 | 0.4851 |
| Number of distal anastomosis | 2.6 ± 0.9 | 2.5 ± 0.9 | 0.4180 | |
| Valve surgery | 26 (29%) | 72 (54%) | 0.0002 | 0.1111 |
| EuroSCORE | 2.6 ± 2.3 | 4.4 ±2.7 | 0.0001 | |
Patient Outcomes
| Rigid Fixation | Conventional Closure | ||
|---|---|---|---|
| Group R | Group C | ||
| Number of patients | 89 | 133 | P value |
| Intubation (hours ± std) | 13 ± 20 | 39 ± 97 | 0.0030 |
| Intubation over 24hours | 3 (3%) | 28 (21%) | 0.0002 |
| Intensive care unit stay (hours ± std) | 58 ± 40 | 99 ± 119 | 0.0003 |
| Intensive care unit stay over 48hours | 56 (63%) | 96 (72%) | 0.1456 |
| Postoperative stay (days ± std) | 7.0 ± 3.7 | 8.4 ± 4.7 | 0.0141 |
| Postoperative stay over 7days | 36 (40%) | 71 (53%) | 0.0587 |
| Major complication (n, %) | |||
| Heart failure | 0 | 0 | 1.0000 |
| Postoperative myocardial infarction | 1 (1%) | 1 (1%) | 0.7739 |
| Ventilator use longer than 48hours | 3 (3%) | 18 (14%) | 0.0112 |
| Pneumonia | 1 (1%) | 5 (4%) | 0.2353 |
| Cerebral vascular accident | 0 | 5 (4%) | 0.0643 |
| Re-exploration for bleeding | 1 (1%) | 0 | 0.2205 |
| Postoperative hemodialysis | 1 (1%) | 1 (1%) | 0.7739 |
| Sternal infection | 1 (1%) | 0 | 0.2205 |
| Inhospital Death | 1 (1%) | 4 (3%) | 0.3356 |
Results of Univariate and Multivariate Analyses for Intubation Time, ICU Stay and Postoperative Length of Stay
| Intubation Time | Multivariate | ICU Stay | Multivariate | Postop Stay | Multivariate | |
|---|---|---|---|---|---|---|
| Univariate | Univariate | Univariate | ||||
| Age under 65 | 0.0014 | 0.4686 | ||||
| Renal dysfunction Cr over 1.5 | 0.0490 | 0.6462 | 0.0114 | 0.6242 | 0.0443 | 0.3116 |
| Preoperative heart failure | 0.0010 | 0.7409 | 0.0012 | 0.6690 | 0.0010 | 0.4402 |
| Emergent or urgent surgery | 0.0165 | 0.2529 | 0.0124 | 0.0596 | ||
| Valve surgery | 0.0034 | 0.9096 | 0.0515 | 0.7022 | ||
| Rigid fixation | 0.0001 | 0.0158 | 0.0158 | 0.0086 | 0.0048 | 0.0642 |
Postoperative outcomes are shown in Table 2. Sternal infection was observed in 1 patient (1%) in group R and none in group C. On exploration of this patient with sternal infection, we found the sternum was still intact with the plates; however, the sternocostal cartilage had completely separated from the sternum. There was postoperative bleeding, which was not related to the sternal closure. The patient required emergent sternotomy at bedside. During the exploration the middle part of the plate was able to be cut using a conventional wire cutter without any delay. The sternum was reclosed in the operating room with the Sternalock using different plating configurations.
Intubation time (13 ± 20 hours vs 39 ± 97 hours, p=0.0030), ICU stay (58 ± 40 hours vs 99 ± 119 hours, p=0.0003), and postoperative length of stay (7.0 ± 3.7 days vs 8.4 ± 4.7 days, p<0.0141) were significantly shorter in group R than group C. On univariate analyses, age greater than 65, elevated preoperative creatinine greater than 1.5 mg/dl, heart failure, urgent or emergent status of surgery, valve surgery, and ridgid fixation were identified to be factors influencing the intubation time, ICU stay and postoperative length of stay (Table 3). Multivariate analyses showed ridgid sternal fixation was the single isolated factor affecting both intubation time and ICU stay, although postoperative length of stay was not affected by the method of sternal fixation.
DISCUSSION
Our retrospective study clearly showed that the application of the rigid fixation was clearly biased. Surgeons preferably chose rigid fixation rather than wire circulage if the patient was at high risk for sternal dehiscence especially in obese patients. Obesity is a major risk factor for sternal dehiscence and infection, [11] which may be related to the inability of close the sternum in an adequate manner by conventional wire circulage. Sternal wire may not be strong enough to hold against stress applied to the sternum when a large person coughs. Broken wires are often observed in obese patients. We consider that rigid fixation in obese patients provides better sternal stability than wire circulage. For same reason, patients who wish to go back to work, especially muscular work, as soon as possible after discharge from hospital, may request rigid fixation. The frequent use of rigid fixation in the patients who have undergone CABG could be due to the concern regarding sternal ischemia from the internal mammary artery harvest.
Low risk patients were also closed with Sternalock system in our institution. The sternum of young patients was more frequently closed with rigid fixation and old patients more frequently closed with wires due to high incidence of osteoporosis among elderly patients. For a similar reason, female patients more often underwent wire closure instead of rigid closure. The osteoporotic sternum can not hold the screw to attach the plate. Poor quality of bone is one of the contraindications for Sternalock use. Thus, sternal wire closure was more frequently used instead. Unfortunately, osteoporosis of the sternum is a subjective judgment of the surgeon and the data were not collected in this study.
The thickness of the sternum is important when performing rigid closure using the Sternalock system. The screw size was selected based on the thickness of the sternum. In our practice, surgeons are encouraged to secure the screw into both the anterior and posterior cortex of the sternum. To ensure this, sternal thickness plus 4 mm is our standard for determining screw size. Since the premade screw size ranges from 8 mm to 16 mm, the minimum thickness of the sternum closed with a Sternalock system is 4mm and maximum thickness of the sternum is 14 mm. A screw that is too long may injure the mediastinal structures, although we have not encountered such a complication. On the contrary, a screw that is too short may become loose, eventually migrate to the subcutaneous tissue, and loose the advantage of rigid closure of the sternum. The plate and screws are made of titanium, thus patients the Sternalock plating may safely undergo magnetic resonance imaging study. However, patients with a titanium metal allergy are not considered the Sternalock sternal closure.
Our postoperative results showed low overall complication rates in both groups. There was one sternal infection in the rigid fixation group, requiring removal of the entire plate. Interestingly, despite the infection, stability of the sternum was maintained. There was no sternal dehiscence but dislocation of the sternocostal cartilage was observed. This indicates that rigid fixation can not completely eliminate the risk of the infection.
Regarding postoperative recovery, early extubation and shorter ICU stay in the rigid sternal fixation group was remarkable. Although selected patients were closed with rigid fixation, multivariate analyses showed the rigid fixation was an independent factor that shortened intubation and ICU time. We speculate that the rigid closure provided secure sternal stability and these patients experienced less pain than patients with conventional wire closure. Less pain may result lower narcotics requirement, and may contribute to early extubation in the rigid fixation group. In this study, the pain scores were not collected since this is a subjective measurement and it was difficult to obtain such data in retrospective manner. We consider that better sternal stability provides better sternal comfort, which further contributes to the patient’s early mobilization and shorter recovery time.
A limitation of this study is the non-randomized observational nature of study. The sample size was relatively small to demonstrate any difference in postoperative complication rates, although it was not main purpose of this study. Pain score and the pain medication data were not included study. A prospective randomized study is necessary to identify the true benefit of rigid fixation over conventional wire closure.
SUMMARY
This retrospective study showed rigid sternal fixation was more frequently used in low risk young male patients, or high risk obese patients. Among these selected patients, ridgid sternal fixation was an independent factor contributing to early patient recovery.
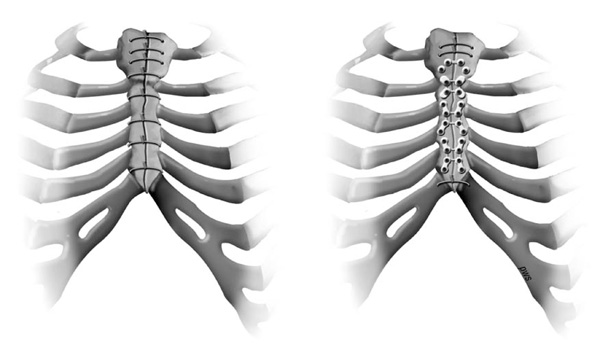
Example of rigid closure of the sternum on the left and conventional wire closure on the right.
CONFLICT OF INTEREST
All authors have no conflict of interest.

