All published articles of this journal are available on ScienceDirect.

Calcified Left Ventricular Aneurysm: “An Egg in the Heart”
Abstract
We present a peculiar case of left ventricular aneurysm which had calcified over 14 years post anterior myocardial infarction and appears to be like an egg in the heart. Previous cases reported of calcified LV ring were associated with Left Ventricular mural thrombus. In our patient, we did not identify any mural thrombus.
MAIN TEXT
A 59 year old gentleman presented with worsening symptoms shortness of breath, orthopnea and increasing ankle swelling. His past medical history included extensive anterior wall myocardial infarction with cardiogenic shock 14 years ago, diabetes mellitus and hypertension. ECG on this admission revealed left bundle branch block and left axis deviation. His chest radiogram revealed a peculiar calcified egg in the heart (Fig. 1). He was treated with digoxin and diuretics which improved his symptoms. His trans-thoracic echocardiogram revealed severely dilated left ventricle with severely impaired systolic function, mild mitral regurgitation and bi-atrial enlargement (Fig. 2). It was difficult to rule out the presence of apical thrombus on his echocardiogram. We performed Cardiac MRI with multi planar black blood and cine white blood images together with delayed post gadolinium enhanced scar imaging. Cardiac MR was done to assess viability and anatomical details of LV aneurysm. This confirmed full thickness scarring in aneurysmal distal apical left ventricle and did not reveal any thrombus at the apex (Fig. 3). The following measurements were obtained: ejection fraction of 10% and stroke volume of 49mls. Contrary to two previously reported cases, our case did not reveal an apical thrombus associated with calcified aneurysm.[1,2] However, he was warfarinzed considering his high thrombo-embolic risk.
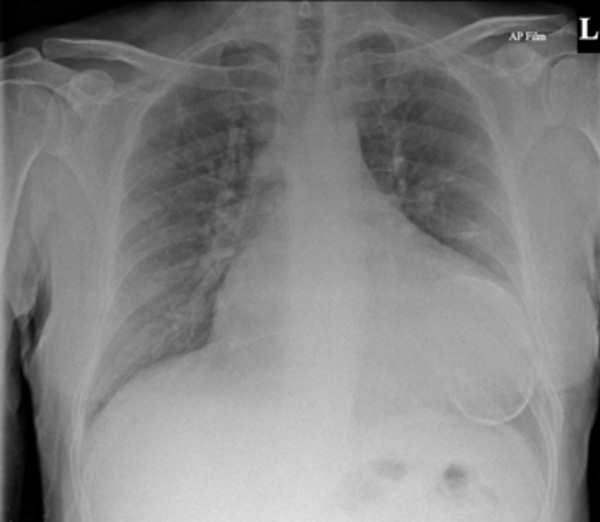
Chest x-ray showing cardiomegaly and an oval shaped calcified structure related to Anterio-apical left ventricular aneurysm.

Transthoracic Echocardiography showing dilated left ventricle and severely reduced ejection fraction. However, mural thrombus could not be ruled out.
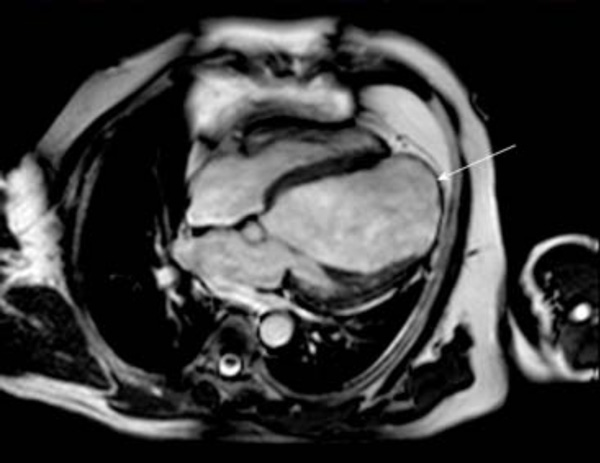
Cardiac MR in four chamber view showing an enlarged left ventricle and apical aneurismal cavity (arrow). No thrombus is seen in LV cavity.

