All published articles of this journal are available on ScienceDirect.

Adult Congenital Heart Disease Investigated with Cardiac Catheterization Over A 20-Year Period
Authors Info & Affiliations
Abstract
Background:
Recent advances in diagnosis and treatment have increased the life expectancy of patients with congenital heart disease.
Methods:
To investigate the prevalence of adult congenital heart disease (ACHD) in a large registry of patients over a 20-year period, we retrospectively assessed data of 14,012 males and 4,461 females who underwent clinically indicated cardiac catheterization from 1984 to 2003.
Results:
ACHD was recorded in 234 subjects aged from 18 to 66 years, [95 males (40.7%) and 139 females (59.3%)]. Females were more likely to present with ACHD than males (p<0.001). Atrial septal defect was the most common defect (43.3%) followed by partial anomalous pulmonary venous return (12.0%), pulmonary valve stenosis (11.3%) ventricular septal defect (8.0%), coarctation of aorta (5.5%) patent ductus arteriosus (4.0%) and Fallot’s tetralogy (3.3%). Atrial septal defect was more common in females (p<0.01), while pulmonary valve stenosis was more frequent in males (p<0.05). No difference across sexes was found in the other forms of ACHD. Females with ACHD were significantly older than males at the time of catheterization (median age 41 years, interquartile range 26 to 53 years vs. median age 35 years, interquartile range 22 to 48 years, p<0.05).
Conclusions:
In adulthood ACHD is found more commonly in females and is diagnosed later in life than in males. Atrial septal defect is the most prevalent form of ACHD and occurs most commonly in females.
INTRODUCTION
Congenital heart disease is the most common form of congenital human disease with a prevalence of 8 to 10 per 1,000 births [1]. Considerable progress has been made over the last decades in the diagnosis and treatment of congenital heart disease. This has markedly increased the life expectancy and quality of life of patients [2]. More than 95% of children with congenital heart disease can now survive to adulthood and this has created a substantial population of patients with adult congenital heart disease (ACHD) [3]. To provide further insight into the most commonly encountered forms of ACHD in clinical practice, we studied the frequency of ACHD in a large series of adult subjects who underwent cardiac catheterization in our institution over a 20-year period. Furthermore, we sought to investigate possible sex and age differences in the most common categories of ACHD.
MATERIALS AND METHODOLOGY
We retrospectively analyzed data of 14,012 males and 4,461 females who underwent clinically indicated cardiac catheterization in the Haemodynamic Laboratory of the 1st Cardiology Department, AHEPA University General Hospital, Thessaloniki, Greece from January 1st, 1984 to December 31st, 2003. Diagnosis of ACHD was confirmed by visual evaluation of all angiograms by an independent expert interventional cardiologist blinded to the patients’ clinical and laboratory records. The Institutional Medical Ethics Committee approved the study.
Categorical variables were summarized as absolute values and percentages. Comparisons between them were carried out using Pearson’s chi-square test and Fisher’s exact test and were expressed as p values and odds ratios (OR) with the corresponding 95% confidence intervals (95% CI). Age was the only continuous variable recorded and as it did not fulfill the assumption of normality, was summarized as the median with the 25th and the 75th percentile of its distribution. Age differences were assessed with Mann-Whitney test. A value of p<0.05 was considered significant. The statistical analyses were performed using SPSS, version 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
ACHD was recorded in 234 out of 18,473 subjects (1.3% of the total population) aged from 18 to 66 years. Of these, 95 were males (40.7%), representing 0.7% of the total number of males (age range from 18 to 64 years), whereas 139 were females (59.3%), representing 3.1% of the total number of females (age range from 18 to 66 years). ACHD was more prevalent in females than in males (females/males OR 4.71, 95% CI 3.62 to 6.13, p<0.001, Fig. 1).
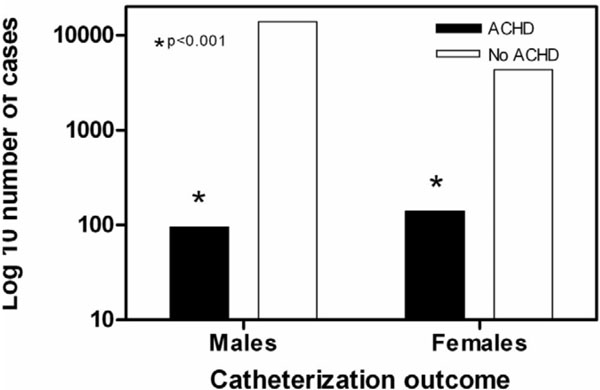
Frequency of adult congenital heart disease (ACHD) in relation to sex. The number of cases is expressed in a logarithmic scale. ACHD was more frequent in females.
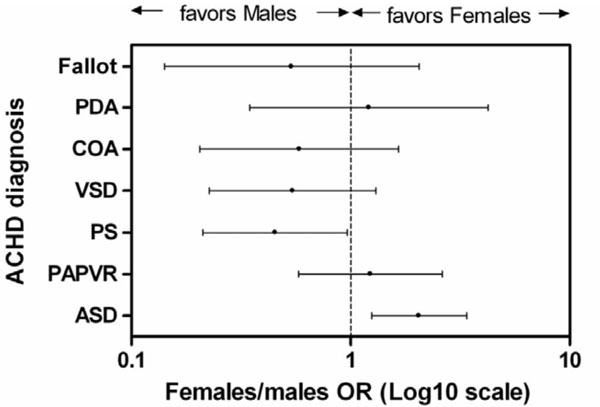
Females/males odds ratio (OR) plot for each type of ACHD. Each point in the graph represents an OR, while the error bars correspond to its 95% confidence intervals (95% CI). An OR with 95% CI>1.0 indicates significantly higher likelihood for females, whereas an OR with 95% CI <1.0 indicates significantly higher likelihood for males. Atrial septal defect was more common in females. Pulmonary valve stenosis was more common in males. Abbreviations: ASD: Atrial septal defect, COA: coarctation of aorta, Fallot: Fallot’s tetralogy OR: odds ratio, PAPVR: Partial anomalous pulmonary venous return, PDA: Patent ductus arteriosus, PS: Pulmonary valve stenosis, VSD: Ventricular septal defect.
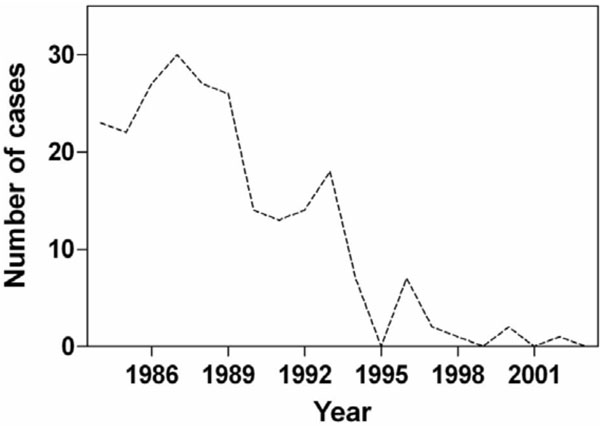
Number of cases with ACHD diagnosed per year throughout the study period.
In 199 cases (85%) a single congenital heart defect was revealed, whereas in 29 cases (12.4%) 2 concomitant heart defects were found and in 6 (2.6%) cases complex ACHD with 3 or more anomalies was present.
With regards to diagnosis, atrial septal defect was the most common anomaly (43.3%) followed by partial anomalous pulmonary venous return (12.0%), pulmonary valve stenosis (11.3%), ventricular septal defect (8.0%), coarctation of aorta (5.5%) patent ductus arteriosus (4.0%) and Fallot’s tetralogy (3.3%; Table 1).
Frequency of the Specific Types of Congenital Heart Disease in Our Registry
| Type of Congenital Heart Disease | Number of Subjects | % | Number of Males | % | Number of Females | % | p |
|---|---|---|---|---|---|---|---|
| Atrial septal defect | 119 | 43.3% | 37 | 33.0% | 82 | 50.3% | <0.01 |
| Partial anomalous pulmonary venous return | 33 | 12.0% | 12 | 10.7% | 21 | 12.9% | ns |
| Pulmonary valve stenosis | 31 | 11.3% | 18 | 16.1% | 13 | 8.0% | <0.05 |
| Ventricular septal defect | 22 | 8.0% | 12 | 10.7% | 10 | 6.1% | ns |
| Coarctation of aorta | 15 | 5.5% | 8 | 7.1% | 7 | 4.3% | ns |
| Patent ductus arteriosus | 11 | 4.0% | 4 | 3.6% | 7 | 4.3% | ns |
| Fallot’s tetralogy | 9 | 3.3% | 5 | 4.5% | 4 | 2.5% | ns |
| Other | 35 | 12.7% | 16 | 14.3% | 19 | 11.7% | ns |
Fig. (2) shows the odds ratios for each type of ACHD across sexes. Atrial septal defect was more prevalent in females (females/males OR 2.05, 95% CI 1.25 to 3.38, p<0.01), whereas pulmonary valve stenosis was more frequent in males (females/males OR 0.45, 95% CI 0.22 to 0.97, p<0.05). The frequency of the other forms of ACHD showed no difference across sexes.
The median age of subjects with ACHD was 38.5 years, interquartile range 25 to 51 years. Females with ACHD were significantly older than males at the time of catheterization [41 (26 to 53) years vs 35 (22 to 48) years, p<0.05].
The number of cases diagnosed per year progressively declined throughout the study period (Fig. 3).
DISCUSSION
This study showed that ACHD is more prevalent in females and this is consistent with previous reports [4,5]. Atrial septal defect was the most common form of ACHD in our series and this is also in agreement with reports from Europe and North America [4-6]. This finding may be attributed to the fact that most commonly atrial septal defect produces less and slowly progressing hemodynamic complications so that more individuals with this condition survive to adulthood. Interestingly the second most common form of ACHD in our series was partial anomalous pulmonary venous return for which we have found no preceding data with regards to frequency. Pulmonary valve stenosis was recorded as the third most common form of ACHD with a total frequency of 11.3% which is higher than existing data [5, 6]. Also, the frequency of ventricular septal defect in our series was considerably lower than what was previously published which ranged from 14% to 19% of the total congenital heart defects [4-6]. With regards to coarctation of aorta, our reported frequency of 5.5% lies within the range of earlier studies that however exhibit high variation with prevalence rates from 1.7% to 13% [4, 5]. The frequency of patent ductus arteriosus in our series (4.0%) was higher than in other registries which was 1.3% or lower [5,6]. Our results concerning the frequency of Fallot’s tetralogy (3.3%) are lower than literature reports which range from 4.2% to 19.7% [4-6].
Another interesting finding in our study is that the age of ACHD diagnosis was higher for females. This could be attributed to the high frequency of atrial septal defect in our series which was more prevalent in females. As atrial septal defect produces milder symptoms than other forms of ACHD it could be assumed that it was diagnosed later in life, thus favoring a higher age of diagnosis for females. A higher age for women with ACHD has been reported in another study but it did not reach significance [6].
With regards to sex differences in specific congenital heart defects, our finding of a higher frequency of atrial septal defect among females was confirmed by previous reports [4-6]. On the other hand, the higher likelihood of males to present with pulmonary valve stenosis has not been previously reported. Defects mainly involving the inflow tract of the heart predominate in females, whereas defects of the outflow tract prevail in males [7, 8]. In this context, it would be expected for atrial septal defect to be more frequent in females and for pulmonary valve stenosis in males, as we report.
Finally, our finding of a reduction of the total number of cases diagnosed with ACHD in the second half of our study (from 1994 to 2003) should not be interpreted as a decline in the prevalence of ACHD. On the contrary, the frequency of ACHD has been reported not to exhibit substantial temporal or geographic variation [9]. Thus, the above result could be attributed to the increased use of non-invasive methods (i.e. echocardiography, computed tomography, magnetic resonance imaging) [10,11] which has limited the indications for diagnostic cardiac catheterization.
Several limitations apply to our study. As it was confined to a specific population consisting of patients referred for cardiac catheterization, the real prevalence of the specific forms of ACHD in the general population could not be assessed. Also, it was conducted in a tertiary care center and many patients were examined upon referral, thus a referral bias relating to the severity of clinical presentation of ACHD cannot be ruled out. Moreover, the diagnosis of ACHD was based solely on data from cardiac catheterization, although newer non-invasive imaging modalities have been proved highly accurate and more easily applicable [10, 11]. This may have introduced a sampling bias in the later years of the study as it is likely that only certain cases of ACHD (potentially those with more clinically significant defects requiring surgical treatment) underwent cardiac catheterization. Detailed information on the medical history of the subjects was not available due to heterogeneity of cases studied in terms of the cardiology center they were referred from and absence of electronic patient records in the first years of the study. Finally, the unavailability of follow up data did not permit us to evaluate the long-term outcome of ACHD.
CONCLUSIONS
In this study ACHD was more prevalent in females and was diagnosed later in life than in males. Atrial septal defect was the most common form of ACHD followed by partial anomalous pulmonary venous return. The large number of subjects enrolled in our registry as well as the extensive time period it covers is an advantage.

