All published articles of this journal are available on ScienceDirect.

Risk Factor Patterns for Premature Versus Late-Onset Coronary Artery Disease in Iran: A Systematic Review and Meta-Analysis
Authors Info & Affiliations
Abstract
Background:
There are few data regarding the risk factors of premature vs late-onset Coronary Artery Disease (CAD). This study systematically reviews these risk factors in Iranian people.
Methods:
Medline, Web of Science, Embase and SID (Scientific Information Database; www.sid.ir) databases were searched for studies comparing CAD risk factors in young and older patients in Iran. Data extracted and pooled odds ratio (OR) with 95% Confidence Interval (CI) for each risk factor were calculated. Publication bias was evaluated by Egger’s test.
Results:
Seven studies (9080 participants) were included in the meta-analysis; analysis was carried out independently for each risk factor. Smoking (Odds Ratio (OR): 2.57, 95% CI: 1.96-3.37; p=<0.001), family history of CAD (OR: 2.45: 95% CI, 1.44-4.15, p<0.001), opium abuse (OR: 2.44: 95% CI, 1.22-4.88; p=0.001) and hyperlipidaemia (OR: 1.4: 95% CI, 1.13-1.73; p=0.001) were more common in premature CAD compared with older CAD patients. In contrast, diabetes mellitus (OR: 0.54: 95% CI, 0.39-0.73; p=0.0001) and hypertension (OR: 0.36, 95% CI: 0.21-0.59; p<0.001) were less prevalent.
Conclusion:
Risk factors were significantly different between premature and late-onset CAD. Policies regarding smoking and opium cessation and controlling hyperlipidaemia may be useful for the prevention of premature CAD in Iran.
1. INTRODUCTION
Although the elderly comprise the majority of patients with Coronary Artery Disease (CAD), the proportion of young patients presenting premature CAD is growing [1]. Young adults may be neglected in cardiovascular (CV) research. This growing group is exposed to various CAD risk factors [2]. Unhealthy diet, obesity, smoking and illegal drug use are factors that should be confronted [3]. Since different CV risk factors patterns exist for premature and elderly groups [4], recognition of such patterns in youths is important and could improve public health management. It was reported that arterial hypertension, abdominal circumference and sedentary life style are becoming more prevalent among elders [5]. Considering the high prevalence of CV disease (CVD) among Iranians and in order to provide a clearer picture for healthcare managers /policy makers, we compared the prevalence of different CV risk factors in young and older Iranian patients diagnosed with CAD.
2. METHODS
The scientific databases Medline, Web of Science, Embase and SID (Scientific Information Database; www.sid.ir) were systematically searched until October 28, 2017 using the following key terms: coronary disease, coronary artery disease, coronary heart disease, vascular disease, atherosclerosis, arteriosclerosis, risk factors, population at risk and IRAN see Table 1. All retrieved articles were independently checked by 2 reviewers. Articles were checked for title and abstract in a first round. Then, full-text checking was carried out for papers chosen during the first step.
2.1. Inclusion Criteria
Studies that compared risk factors of CAD in young and elderly Iranian patients were included in the present article Table 2. Letters to editors, duplicated articles, congress abstracts and reviews were excluded.
2.2. Data Extraction and Quality Assessment
The following data were extracted by 4 independent reviewers: first author name, year, study population size and age (years), study design, diagnosis criteria of CAD as well as risk factors including smoking, hypertension, diabetes mellitus, opium abuse, family history of CAD, obesity, hyperlipidaemia and lipid profile. Risk factors extracted from the retrieved papers (proportion of patients have/have not a risk factor in young and elder groups in each study for dichotomous variables as smoking, hypertension, diabetes mellitus, opium abuse, family history of CAD, hyperlipidaemia and mean and number of each groups for quantitative variables as lipid profile and body mass index) included in our meta-analysis are reported in Table 3. In this study, we used Joanna Briggs Institute Critical Appraisal Checklist to evaluate the quality of case control, cross-sectional and cohort studies. Each retrieved article was independently evaluated by 2 reviewers using the above noted checklist and a joint decision was made for inclusion/exclusion of each article. In case a joint decision could not be achieved, a third reviewer checked the article.
2.3. Statistical Analysis
STATA ver.11 was used to analyse data for each risk factor. The Odds Ratio (OR) with 95% Confidence Interval (CI) was calculated for each risk factor and results from the selected studies concerning the risk factors hyperlipidaemia were analysed using the fixed effects model, while the random-effects model (DerSimonian and Laird method) was used for analysing results on diabetes mellitus, smoking, hypertension, family history and opium abuse. Study heterogeneity was evaluated by I2 (an estimate of the variance across studies caused by heterogeneity rather than chance). Sensitivity analysis was carried out to assess the robustness of pooled estimates if appropriate [6, 7]. Publication bias was assessed by Egger test.
3. RESULTS
3.1. Study Characteristics
Searching Medline, Web of Science, Embase and SID databases yielded 2866 potential papers, of which, 10 papers were eligible for meta-analysis. However, risk factors that were discussed only by 1 study were not included in the meta-analysis. Finally, meta-analysis was performed for 7 studies including cross sectional [8-11], case control [12] and cohort studies [13, 14], with 9080 subjects (Fig. 1). Meta-analysis was separately carried out for each risk factor of premature CAD according to data reported in papers and 3 to 6 papers were included in meta- analysis for each risk factor depending on the reported data. Table 1 demonstrates qualitative reports of studies eligible for meta-analysis.
The definition of young and elderly CAD varied among studies; 1 study considered those aged <50 years for men and 55 years for women as “young” [13]; others considered 35 [8], 45 [15], 50 [9], 55 [12], 60 [14] and, 45 years old as “young” and >65 years old as “older” [10].
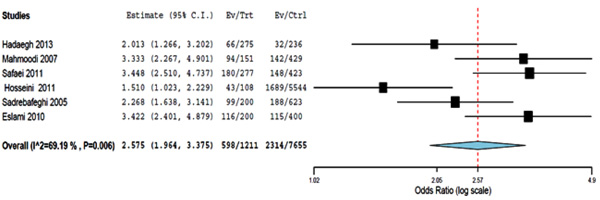
3.2. Smoking
Six studies investigated the association between smoking and CAD in young and elderly patients. In young patients, smoking was associated with a higher risk of CAD compared with elderly CAD patients (OR: 2.57: 95% CI, 1.96-3.37; p≤0.001), with a heterogeneity of I2=69.1% among the studies (p=0.006) (Fig. 2). Sensitivity analysis did not affect the results. No publication bias was found in the evaluated articles (Egger test, p=0.5).
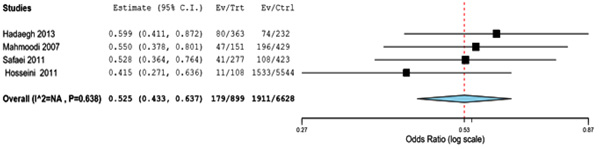
3.3. Diabetes Mellitus
Six studies investigated the association between diabetes mellitus and CAD in young and elderly patients. Diabetes mellitus was associated with a lower risk of CAD in young patients compared with elderly patients (OR: 0.54: 95% CI, 0.39-0.73; p<0.001). Statistically significant heterogeneity was found among the studies (I2= 71.35%; p=0.0.004) (Fig. 3) and no publication bias was seen (Egger test, p=0.05). In sensitivity analysis after deletion of one study [13] the result did not have heterogeneity.
3.4. Hyperlipidaemia
Three studies compared the frequency of hyperlipidaemia in young and elder CAD patients. Hyperlipidaemia was associated with a higher risk of CAD in young patients compared with elderly patients (OR: 1.4: 95% CI, 1.13-1.73; p=0.002). No statistically significant heterogeneity was found among the studies (I2= 0%; p= 0.7) (Fig. 4) and no publication bias was detected (Egger test, p=0.2).
| Database | Search Strategy | Result |
|---|---|---|
| Medline | (“coronary disease” OR “coronary diseases” OR “coronary artery disease” OR “coronary artery diseases” OR “coronary heart disease” OR “coronary heart diseases” OR “vascular disease” OR “vascular diseases” OR “atherosclerosis”) AND (“risk factor” OR “risk factors” OR “population at risk” OR “populations at risk”) AND Iran | 831 |
| Embase | (“coronary disease” OR “coronary diseases” OR “coronary artery disease” OR “coronary artery diseases” OR “coronary heart disease” OR “coronary heart diseases” OR “vascular disease” OR “vascular diseases” OR “atherosclerosis”) AND (“risk factor” OR “risk factors” OR “population at risk” OR “populations at risk”) AND Iran | 2402 |
| Web of Science | (“coronary disease” OR “coronary diseases” OR “coronary artery disease” OR “coronary artery diseases” OR “coronary heart disease” OR “coronary heart diseases” OR “vascular disease” OR “vascular diseases” OR “atherosclerosis”) AND (“risk factor” OR “risk factors” OR “population at risk” OR “populations at risk”) AND Iran | 285 |
| overall | - | 3518 |
| Outcome | Cut off for Age of Study population | Study Design | Participants in Premature/late Onset Group, n | Source |
|---|---|---|---|---|
| Cardiovascular disease | 30-60 years vs ≥60 years | cohort | 275 /237 | Hadaegh, 2013 (14) |
| Myocardial Infarction | ≤ 50 vs >50 | Cross sectional | 151/429 | Mahmoodi, 2007 (9) |
| CAD patients underwent CABG | <45 vs >65 | Cross sectional | 277/423 | Safaei, 2011 (10) |
| Acute ST-segment elevation myocardial infarction | ≤35 vs >35 | Cross sectional | 108 /5544 | Hosseini, 2011 (8) |
| Angiographic documented CAD | <55 vs ≥55 | case control | 103 / 110 | Vaisi-Raygani, 2010 (12) |
| Myocardial Infarction | (Women ≤55 Men ≤50) vs (Women >55 men >50 |
cohort | 200/623 | Sadrebafeghi, 2005 (13) |
| CAD (ICD-10): I20-I25 | ≤45 vs >45 | Cross sectional | 200 /400 | Soleimani, 2010 (11) |
| Risk Factor | Definitions in Papers |
|---|---|
| Diabetes | 1- Mahmoodi (2007): Diabetes mellitus was defined as fasting blood glucose levels >125 mg/dL or a history of diabetes in the past or present with or without medication use at the time of admission 2- Hadaegh (2013): Diabetes mellitus was defined as fasting plasma glucose (FPG) level ≥7 mmol/L and the current use of anti-diabetic drugs 3- Hosseini (2011): symptoms of diabetes and plasma glucose concentration ≥ 200 mg/dl (11.1 mmol/l), or fasting blood sugar (FBS) ≥ 126 mg/dl (7.0 mmol/l) or after 2-h ≥ 200 mg/dl (11.1 mmol/l) 4- Safaei (2011): Not defined in the paper |
| Hyperlipidaemia | 1- Mahmoodi (2007): Hyperlipidaemia was defined as documented history with or without use of antilipidaemic drugs or having cholesterol levels >200 mg/dL or triglyceride level >150 mg/dL or both 2- Sadrebafeghi (2005): Hyperlipidaemia was defined as history of antilipidaemic drugs or cholesterol levels >200 mg/dL or triglyceride level >150 mg/dL or LDL>160 5- Safaei (2011): Not defined in the paper |
| Hypertension | 1- Mahmoodi (2007): Hypertension was defined as a history of HTN in the past or blood pressure ≥140/90 mmHg with or without antihypertensive medication at the time of admission 2- Safaei (2011): SBP of 140 mmHg or higher DBP of 90 mmHg or higher or current use of antihypertensive medication 3- Sadrebafeghi (2005): documented history of hypertension or antihypertensive drug 4- Hosseini (2011): systolic blood pressure ≥140 and/or diastolic ≥90 mmHg and/or on anti-hypertensive treatment 5- Vaisi-Raygani (2010): Hypertension was defined as resting systolic blood pressure ≥160 mmHg and diastolic blood pressure ≥95 mmHg or used anti hypertension drugs. 6- Soleimani (2010): Not defined in the paper |
| Smoking | 1- Hadaegh (2013): Smoking status was defined on the basis of response to the smoking behaviour questions: those who have never smoked, former smokers and current smokers. 2- Mahmoodi (2007): Smoking habit was ascertained by questionnaire and defined as current smoker and never smoked 3- Hosseini (2011): patient regularly smokes a tobacco product/products one or more times per day or has smoked in the 30 days prior to admission 4- Sadrebafeghi (2005): History of smoking >10 cigarettes/day in 3 months 5- Safaei (2011): Not defined in the paper 6- Soleimani (2010): Not defined in the paper |
| Family history of CAD | 1- Hadaegh (2013): Family history of premature CVD reflected any prior diagnosis of CVD in female first-degree relatives, aged less than 65 years or male first-degree relatives under the age of 55 years old. 2- Mahmoodi (2007): Family history was defined as MI history in one parent or both. 3- Hosseini (2011): first degree relatives before the age of 55 years in men and 65 years in women 4- Safaei (2011): Not defined 5- Soleimani (2010): Not defined |


3.5. Hypertension
Six studies compared the frequency of hypertension between young and elder CAD patients. Hypertension was associated with a lower risk of CAD in young patients compared with elderly patients (OR: 0.36: 95% CI=0.21-0.59; p<0.001). Significant heterogeneity was detected among the studies (I2=89%; p<0.001) (Fig. 5). In sensitivity analysis, exclusion of the Vaisi-Raygan study, showed that the remaining studies were homogenous (OR=0.45: 95% CI=0.4-0.51; p<0.001). No publication bias was found (Egger test, p=0.66)
3.6. Family History of CAD
Five studies investigated the association between family history and CAD in young and elderly patients. Family history of CAD was significantly associated with a higher risk of CAD in young patients compared with older subjects (OR: 2.45: 95% CI, 1.44 -4.15; p<0.001). A significant heterogeneity was found among the studies (I2=84%; p<0.0001) (Fig. 6). In sensitivity analysis, following exclusion of the Safaiee et al. study, studies were found to be homogenous (OR: 1.91, 95% CI= 1.37-2.66, p<0.001 and I2=53%, p=0.08) which might be due to large difference between the “age cut-off” considered by Safaiee et al. for young (i.e. <45 years old) and older patients (>65 years old). No publication bias was found (Egger test, p=0.5).
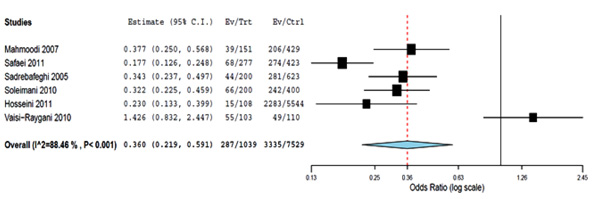
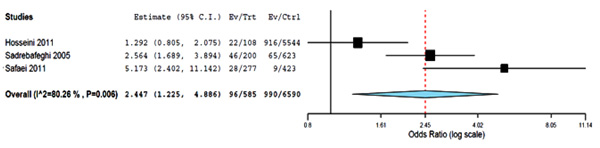
3.7. Opium Abuse
Three studies investigated the association between opium abuse and premature CAD and late onset CAD. Opium abuse was associated with higher risk of premature CAD compared with late onset CAD (OR: 2.44: 95% CI=1.22-4.88; p=0.01). A significant heterogeneity was found among the studies (I2= 80.2%; p=0.006) (Fig. 7). No publication bias was detected (Egger test, p=0.7).

4. DISCUSSION
In this systematic review and meta-analysis, the prevalence of certain CV risk factors varied significantly between Iranian patients with premature and late-onset CAD. Opium abuse, smoking, hyperlipidaemia and family history of CAD are more frequent in premature CAD compared with late-onset CAD; however, diabetes mellitus and hypertension were more frequent in late-onset CAD.
Similar to other studies, we found that smoking was more prevalent in premature CAD compared with late-onset disease [1, 16, 17]. Smoking initiates/promotes atherosclerosis by altering cardiac haemodynamics, dyslipidaemia and increased free oxygen radicals [17]. Smoking is associated with lower High Density Lipoprotein Cholesterol (HDL-C) levels, higher triglycerides, unfavourable changes in apolipoprotein (apo) A1 and B, and in lipoprotein particle size [18]; the apoB/apo A ratio predicts CV events [19]. Compared with non-smokers, cigarette smoking was found to be associated with an average lifetime loss of 10 years [20]. One year after the implementation of smoking restriction in public and hospitality sectors in Germany, a decline of 13.3 and 8.6% in angina pectoris and myocardial infarction, respectively, was reported [21]. Thus, smoking cessation and strategies to prevent smoking relapse should be considered.
We found that the prevalence of opium abuse is significantly higher in young CAD patients compared with older subjects with CAD. Although our analysis showed a significant association between smoking and opium abuse with higher CAD risk in young adults, it should be noted that the vast majority of opium abusers are also cigarette smokers. Nonetheless, Masoomi et al. reported that opium abuse was recognized as a CAD risk factor in non-smokers after adjusting for other CAD risk factors [22]. Prevention programs concerning smoking/illegal substance (e.g. opium) abuse should be planned for young Iranian adults and put into practice in order to minimize the risk such habits pose for CAD.
Our meta-analysis showed that hyperlipidaemia is more prevalent in young CAD patients compared with older patients. However, studies are not consistent in this regard as some studies reported that dyslipidaemia is more prevalent in young patients [23, 24] while others showed that it is more prevalent in older patients with CAD [25-27].
We found that family history of CAD in premature CAD is twice as prevalent as that in late-onset CAD. Andresdottir et al. [28] reported that regardless of cholesterol levels, obesity and hypertension, up to 16.6% of CAD cases are attributable to CAD family history. Women with a history of premature maternal infarction younger than 50 years, showed up to 2.57 fold increased risk of CAD compared with women without such history [29]. Compared with older ST-segment elevation myocardial infarction (STEMI) patients, a family history of early CAD (OR=3.194) was significantly more associated with STEMI in young patients [30].
Similar to other studies, we found that diabetes mellitus prevalence increases with increasing age as diabetes mellitus was less frequent in young compared to older CAD patients [25, 26]. Age-related risk factors, such as diabetes mellitus, are known to be more prevalent in older than younger patients. Risk factors for premature CAD between age- and sex-matched patients and healthy controls are studied elsewhere (data not published yet).
To the best of our knowledge, this study is the first systematic review with meta-analysis regarding CAD risk factors in young Iranian adults. The prevalence and the severity of the risk factors were compared with elder patients. Identification and ranking of prevalent risk factors especially in young adults is of importance for public health systems.
Special concern and attention has been placed by the authors on the low probability power of the Egger test in identifying publication bias in small numbers of studies included in a meta-analysis (current meta-analysis 3-6 studies). More specifically, the power of the Egger method to detect bias is low with small numbers of studies, while the Begg method makes fewer assumptions than the Egger test, but it is insensitive to other types of bias (type 1 and 2 error) to which the Egger test is sensitive [31, 32]. In this meta-analysis all Egger test p values were higher than 0.1 (significant level) except for diabetes mellitus. Nevertheless, our results regarding publication bias are consistent with both tests. Another concern that exits is the competing risk of other risk factors that affect mortality rate at earlier age; in this regard, some patients may have died before becoming “elderly” due to various causes including CAD.
Since the definition of “Premature Coronary Artery Disease” was not consistent across studies, over/under-estimation may occur in pooled analysis of risk factors frequency. Preventive treatment was also not mentioned in all of studies.
CONCLUSION
Opium abuse, cigarette smoking, hyperlipidaemia and family history of CAD were more prevalent in young Iranian CAD patients compared with older ones. It is of crucial importance to conduct large cohort studies in order to establish vascular risk factor among different age groups.
SOURCE OF FUNDING
Mashhad University of Medical Sciences, Mashhad, Iran.
CONSENT FOR PUBLICATION
Not applicable.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

